Xcode Life’s Traits & Personality report profiles genes associated with various personality traits. This report mainly revolves around behavioral genetics, which is a field that analyzes how genes and environments bring about differences in mood, personality, and intelligence.
Some people are predisposed to being open and outgoing, while others may be more shy and reserved. While some may be big risk-takers, a few others may prefer playing it safe. This is because we are predisposed to a certain way of interacting with people around us.
Some interesting facts about genes and personality traits:
Genetics accounts for 34 to 47% variance in empathy
Heritability of leadership role occupancy is about 24%
Up to 42 percent of the tendency to be an entrepreneur is genetic
20% of the variation in educational attainment is genetic
67% of anger trait variation is associated with genetic variability
33% variation in life satisfaction is explained by genetic variations
The report covers over 25 personality traits associated with employment, education, emotion, relationship, and mood. Along with your outcome, the details of the genes analyzed for each trait are also provided. The report comes with personalized recommendations based on your results. These recommendations include tips to enhance or improve your personality.
Please bear in mind that human traits are a result of complex interactions between multiple genes and environmental factors. The findings presented in this report are of a preliminary nature and are not meant for diagnostic purposes.

The report analyzes 25+ personality-related parameters, including empathy, leadership potential, exploratory behavior, creativity, optimism, memory, reaction time, and deep sleep. For a comprehensive list of the traits covered, click here.
For a sample Trait and Personality report/ preview of the report, click here.
The MTHFR and methylation report provides information about the common polymorphisms in the MTHFR gene associated with increased levels of homocysteine, a harmful substance, in the blood.
MTHFR stands for methylenetetrahydrofolate reductase.
MTHFR is a gene that produces the enzyme methylenetetrahydrofolate reductase (MTHFR). This enzyme is responsible for the conversion of inactive folate to active folate. A change in this gene in some people can disrupt this conversion and lead to various health problems. Some signs of MTHFR polymorphisms are cardiovascular and thromboembolic diseases, anxiety, bipolar disorder, colon cancer, and chronic pain.
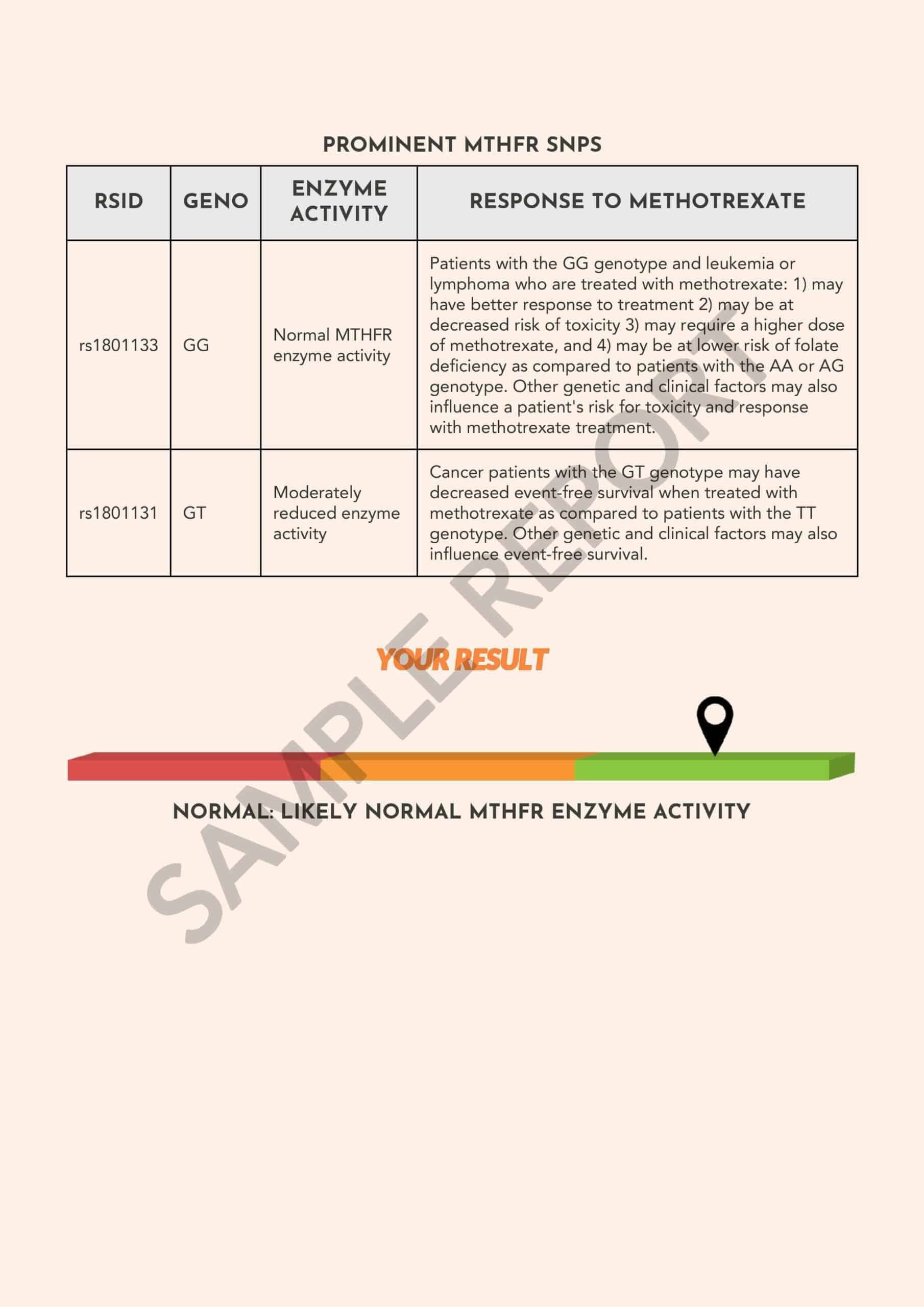
There are two important MTHFR single nucleotide polymorphisms or SNPs, rs1801133, and rs1801131, associated with the MTHFR enzyme activity.
Depending on the genotype of these SNPs, your final result is displayed as a bar diagram.
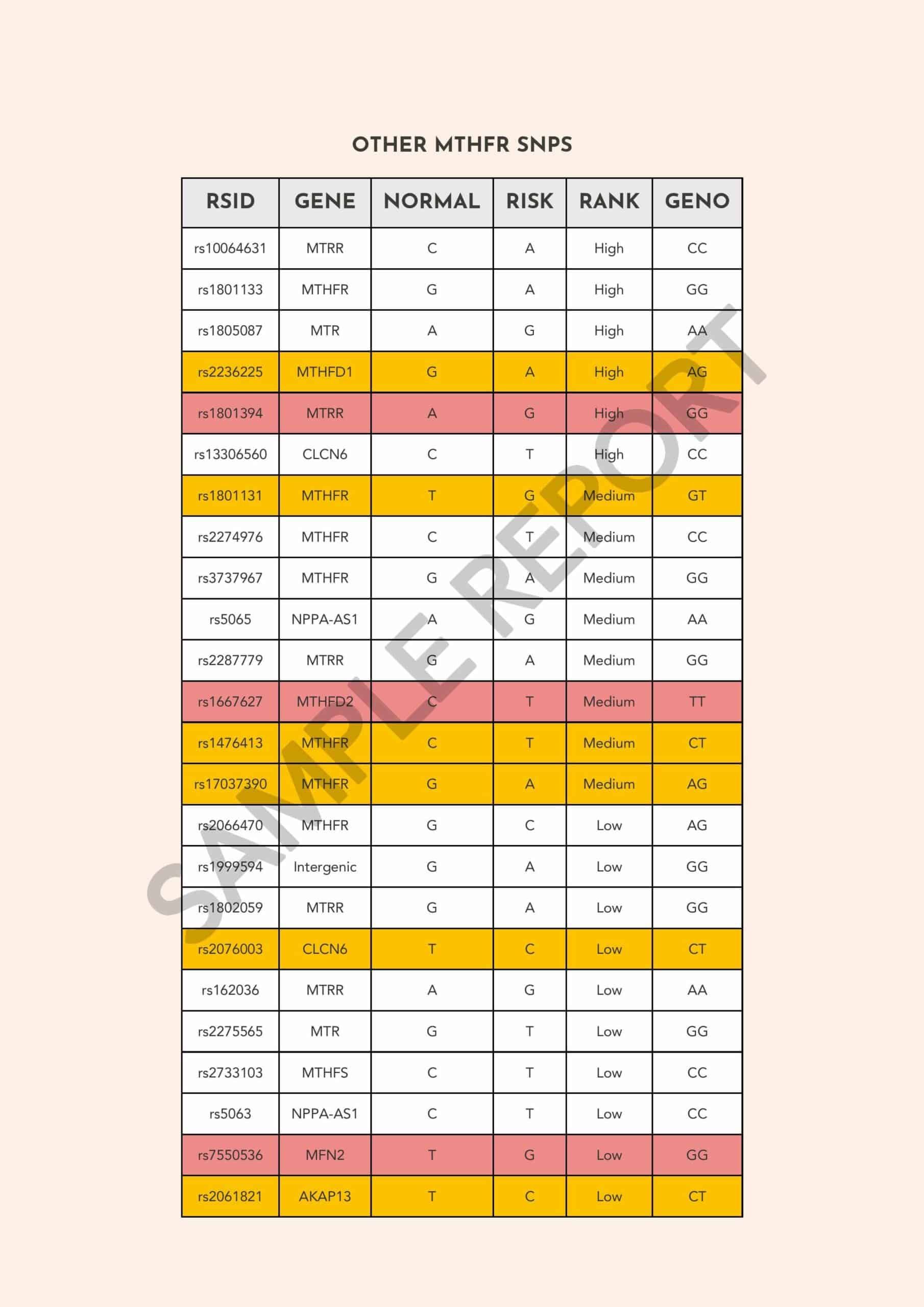
The next section of the report titled “Other MTHFR SNPs” profiles your genotypes for other variations in the MTHFR gene, which are associated, in varying degrees, with MTHFR enzyme activity.
The ‘normal’ column denotes the variant associated with normal enzyme activity, and the ‘risk’ column displays the variant associated with reduced enzyme activity. ‘Geno’ refers to your genotype.
If you carry two risk variants for the SNP, then it is marked in red. If you carry one risk variant, it is marked in yellow, and if you carry two normal variants, it is marked in white.
The ‘Rank’ describes the impact of the SNPs on health. ‘High’ denotes high-impact SNPs with a greater impact on health. Medium and low indicate moderate and lower impacts, respectively. Please bear in mind that the Rank is a theoretical value and not experimentally verified.
One common effect of the mutation is elevated homocysteine levels, which have been linked with conditions such as birth defects, heart diseases, Alzheimer’s, and depression. The final section of the report comes with recommendations targeted at decreasing homocysteine levels. They are to be followed only after consulting with a qualified medical practitioner.
Please bear in mind that human traits are a result of complex interactions between multiple genes and environmental factors. The findings presented in this report are of a preliminary nature and are not meant for diagnostic purposes.
The report analyzes over 15 genes that play a role in methylation, including MTHFR, MTR, MTRR, and NOX4.
For a sample MTHFR report/ preview of the report, click here.
Xcode Life’s BRCA and Breast Cancer Report targets genes that are associated with cancer susceptibility. This report helps you learn about your predisposition to breast and other cancers and take preventive action.
BRCA is an abbreviation for Breast Cancer Gene.
BRCA1 and BRCA2 are the most common genes associated with breast and ovarian cancers. These genes actually help prevent tumor cell formation by repairing any DNA damage. If there are any errors or mutations in these genes, it can increase the risk of several cancers, including breast, ovarian, prostate, and pancreatic cancer.
Testing positive for a BRCA mutation means your risk of developing breast and ovarian cancer is greater than that of the average person. However, higher risk does not imply a diagnosis of cancer.
Xcode Life's BRCA and Breast Cancer Report - $40 - 34 traits
In the Breast Cancer Report, we profile genes that are shown to be associated with an increased risk of breast cancer and your response to various drugs administered for breast cancer.
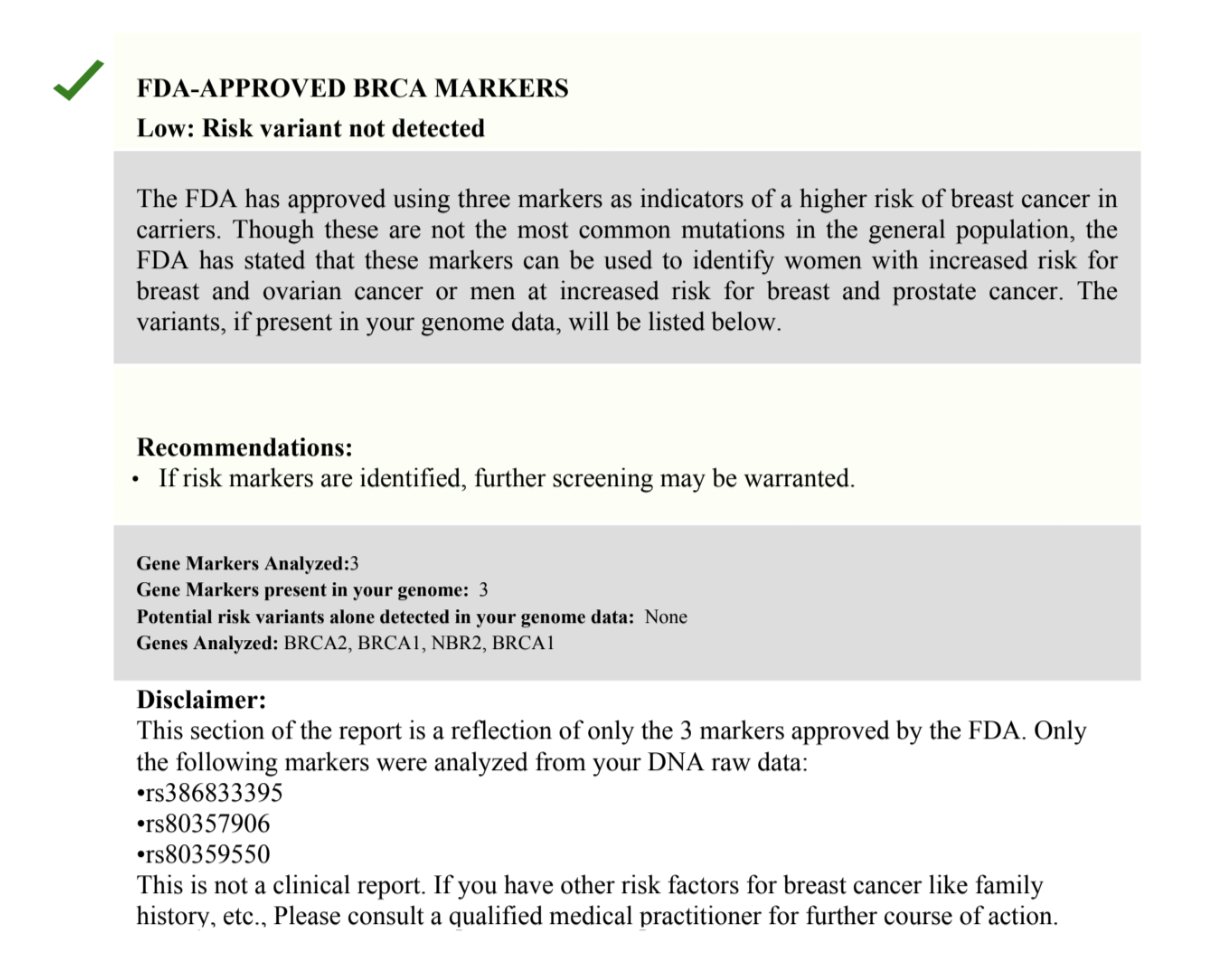
In 2018, FDA approved the genetic testing of 3 specific BRCA gene mutations. Women who test positive for one of the mutations are at increased risk of developing breast and ovarian cancers.
A faulty BRCA1 or BRCA2 gene can be passed down from one generation to the next. In the first section of the report, the three FDA-approved markers and other mutations in the BRCA genes associated with increased cancer risk are analyzed.
55%–72% of women who inherit a harmful BRCA1 variant and 45%–69% of women who inherit a harmful BRCA2 variant will develop breast cancer by 70–80 years of age
People who have a family history of breast cancer are estimated to have at least a one-in-ten chance of carrying a faulty gene.
The report also profiles other genes that indirectly affect the risk of breast cancer. Some examples are genes that affect the expression of estrogen receptors, breast size, and Estradiol Plasma Levels.
Your gene variations also influence breast cancer drug therapy. Understanding your genetic metabolism of various drugs will help you avoid potential adverse events related to ineffectiveness of, or hypersensitivity to the therapeutic agent.
The term ‘Evidence Level’ used here is a parameter that describes the strength of the association between the drugs and the genes implicated.
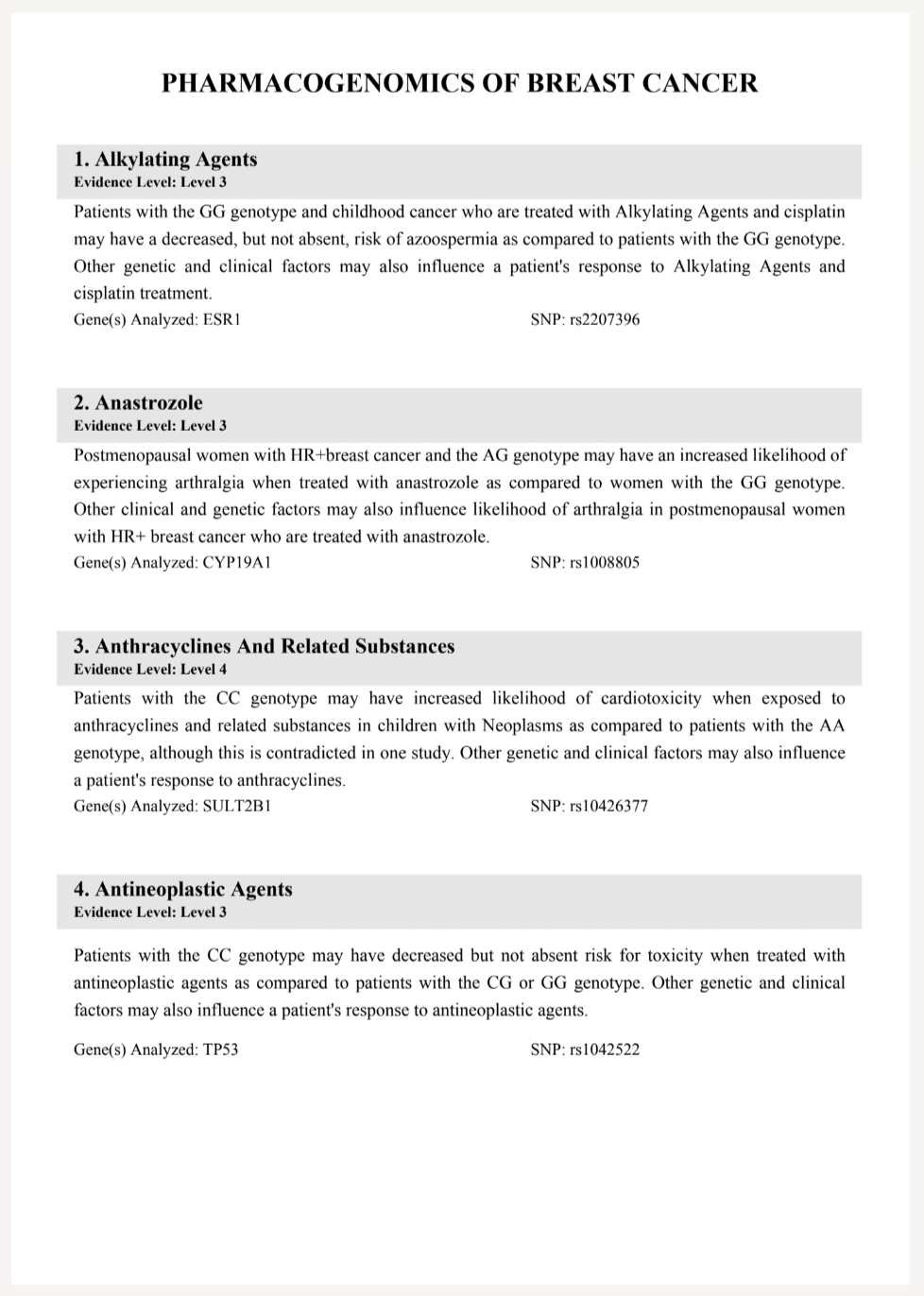
Evidence Level 1A describes the strongest association. This means that the relationship has been established across various studies and approved by guidelines like CPIC. Gene variants under 2A are considered to be Very Important Pharmacogenes by PharmGKB. The Functional significance here is more likely.
Please bear in mind that human traits are a result of complex interactions between multiple genes and environmental factors. The findings presented in this report are of a preliminary nature and are not meant for diagnostic purposes.
The report analyzes 25+ breast cancer-related parameters, grouped under categories like mammographic factors, lifestyle factors, hormonal factors, reproductive lifespan, associated comorbidities, management, and pharmacogenomics. For a comprehensive list of the traits covered, click here.

For a sample BRCA report/ preview of the report, click here.
Vitamin D deficiency is a common health problem worldwide among all age groups. Previous research studies have reported that ultraviolet (UV) exposure causes the skin to produce the hormone endorphin, which is chemically related to morphine, heroin, and other opioids.
A subsequent study reported that UV exposure raises endorphin levels in mice, displaying behavior consistent with opioid addiction. Recent research suggests that vitamin D supplementation may play a role in fighting opioid addiction.
Vitamin D, essential for a range of bodily functions, is predominantly obtained from exposure to sunlight. Once the body takes up vitamin D, it needs to be converted into its active form. Vitamin D is also naturally present in dietary sources like fish liver oils, fortified grains, dairy products, and egg yolks.
Vitamin D deficiency can occur when a person’s skin has an impaired ability to synthesize vitamin D from the sun. Individuals can also become deficient when their bodies cannot absorb the vitamin or convert it to its active form. People who avoid sun exposure, adhere to a vegan diet, or suffer from milk allergies may also be at a higher risk of vitamin D deficiency.
Vitamin D is vital for strong bones as it helps the body use calcium from the diet. Vitamin D deficiency has been associated with rickets, a condition leading to soft bones and skeletal deformities. However, increasing research suggests the importance of vitamin D in protecting against other health problems.
Know more: Genetic Factors That Could Increase Your Risk For Vitamin D Deficiency
Opioids are a form of narcotic prescribed as an over-the-counter pain medication. If incorrectly used, they can have serious side effects and even result in opioid addiction.
Individuals may gain tolerance to opioid medication if taken regularly and might need an increased dose to achieve the same effect in easing pain. They may also develop a dependence on the medication due to extended period use. In this case, individuals who abruptly stop the drug use may experience withdrawal symptoms.
A study led by Dr. David Fisher and his team of researchers at the Massachusetts General Hospital examined the potential link between UV radiation, vitamin D, and opioids.
Initially, the researchers began by studying two data sets.
The researchers drew the following conclusions from the data sets:
These results accounted for factors like age, gender, history of bone fractures, and chronic pain. However, further investigation was required to understand the association between low vitamin D and opioid use.
The researchers used mouse models to understand the patterns seen in the clinical data.
They induced vitamin D deficiency in the mice using the following methods:
50% of the diet-deficient mice were put on a regular diet for eight weeks before examining their response to morphine.
All the mice were then subject to a conditioned place preference (CCP) test in which the mice are placed in a multi-compartment chamber, trained to anticipate morphine in one chamber. Researchers then measured how long the mice spent inside the morphine chamber.
The following were observed:
The team found that the effect was reversed when they restored vitamin D levels using supplements. The researchers confirmed the results with a new batch of mice and additional sensory cues.
Furthermore, the researchers wanted to know whether vitamin D deficiency influenced how mice respond to opioids. For this, they placed control and deficient mice on a hot plate and measured their response to physical pain. Then, the test was rerun after administering the mice with morphine.
Test results reported that vitamin D–deficient mice stayed on the plate longer, implying the morphine worked more effectively as a pain reliever. There was an effect reversal upon vitamin D restoration. Additionally, the heightened pain threshold from a lack of vitamin D disappeared, demonstrating that the effect is opioid-mediated.
Are You Meeting Your Vitamin D Needs? Find out with our Gene Nutrition Report!
The researchers exposed transgenic mice lacking vitamin D receptors to UV. Similar to earlier results, daily exposure to low-dose UV increased pain tolerance in the vitamin D–deficient mice. Findings also show that the mice spent more time in compartments associated with UV exposure, suggesting a lack of vitamin D sensitizes them to the rewarding effects of UV.
The team believes that mice and humans may have evolved molecular pathways to benefit from UV and vitamin D. These pathways induce the same feelings one might get when taking opioids but then control the cravings once vitamin D levels are sufficient.
Previous studies suggest that some people develop an urge to sunbathe and tan, mirroring the behaviors of opioid addicts. Fisher and his colleagues hypothesized that people seek out UV to benefit from an endorphin rush.
In conclusion, vitamin D deficient people would feel compelled to seek out the sun, receiving an endorphin rush. But once their bodies generate enough vitamin D, the endorphin production stops. In the case of opioids, there is no molecular switch to turn off the craving.
The association between vitamin D and opioid response can help with patient care. Checking vitamin D levels before a patient’s surgery could determine whether they are likely to have a heightened tolerance or develop an addiction.
Also read: Will Fish Oil Supplements Help Your Heart Health? Depends On Your Genetic Makeup!

https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4018438/
https://advances.sciencemag.org/content/7/24/eabe4577.abstract
https://www.sciencedaily.com/releases/2021/06/210611174042.htm
Amlodipine is a drug used to treat high blood pressure (hypertension). It belongs to a class of drugs called calcium channel blockers.
The main goal of this class of drugs is to widen the blood vessels and improve the blood flow through them.
When the blood vessels are widened, the pressure applied by the blood on the vessel walls is reduced.
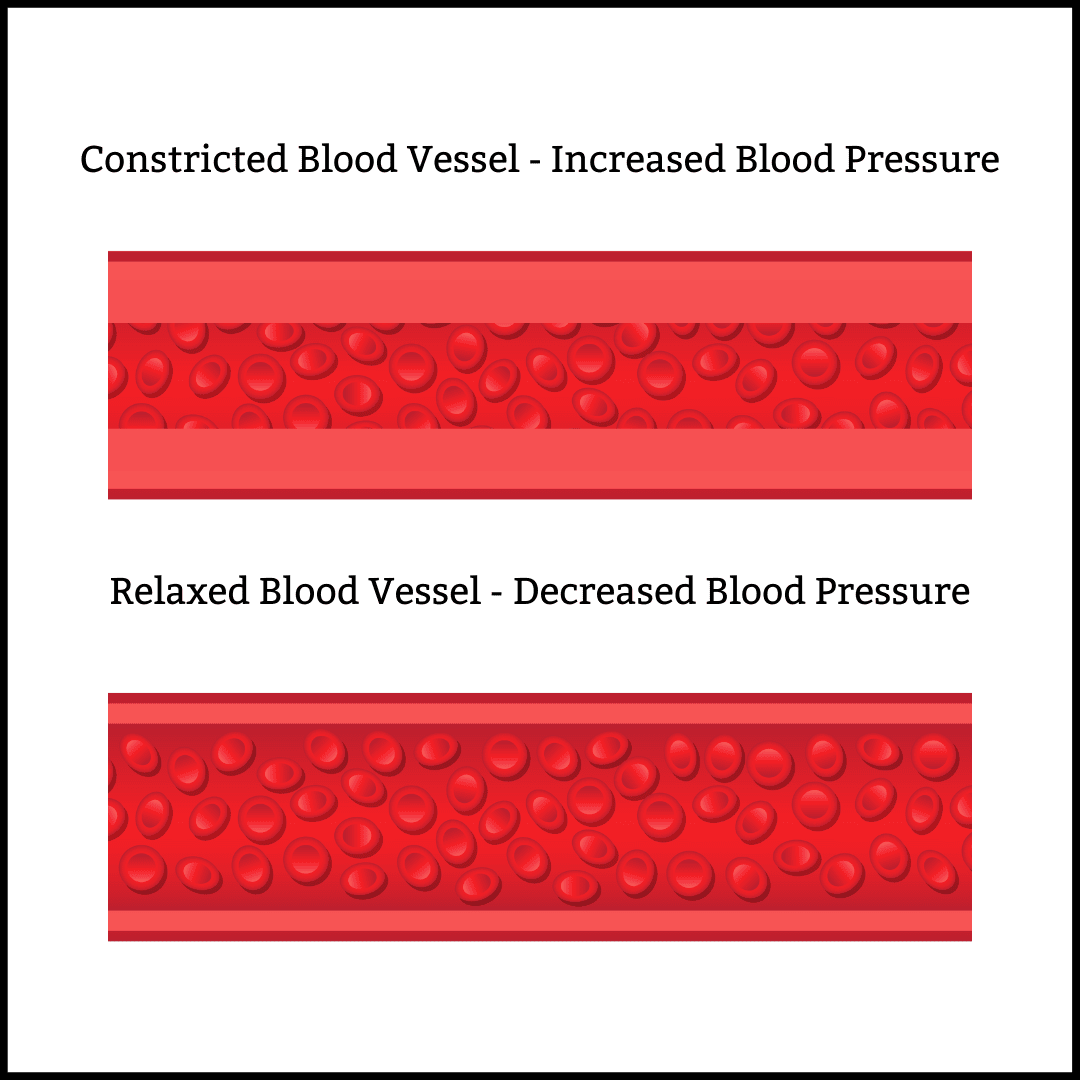
Image: Blood vessels constrictions vs. relaxation and blood pressure
Apart from hypertension, Amlodipine is also used to reduce the frequency of chest pain (angina) and other diseases that affect the blood vessels in the heart.
Amlodipine is usually recommended for adults and children who are at least six years old.
One can take Amlodipine with or without other blood pressure-lowering medications.
Amlodipine is available in the tablet and suspension (or liquid) form that can be taken by mouth (orally).
It is usually recommended to be taken once a day and at the same time each day.
High blood pressure (or hypertension) is a prevalent health condition that can arise from both lifestyle and genetic factors.
Blood pressure is essentially the pressure of circulating blood against the walls of the blood vessels.
If not controlled or treated in time, hypertension can damage other organs in the body such as the brain, kidneys, blood vessels, etc.
Damage to these organs can result in heart disease, heart attack, heart or kidney failure, liver failure, and vision loss.
Medications used to treat hypertension are called antihypertensives and are of different types depending upon their mechanism of action.
Amlodipine belongs to a class of antihypertensives called calcium channel blockers.
This drug primarily acts on the blood vessels and widens their diameter.
Amlodipine blocks calcium entry into smooth muscles of the blood vessels and cardiac muscles.
This allows the blood vessels to relax, improves blood flow through them, and lowers the force of blood on the vessel walls.
As a result, blood pressure levels are reduced.
In most cases, Amlodipine is a safe drug to consume.
However, some side effects of this drug have been noted.
The common side effects of Amlodipine are:
Many of these common side effects may subside within a few days to weeks of taking the Amlodipine.
However, if they do not reduce, consult with your doctor.
Some severe side effects that may occur on taking Amlodipine are:
If you experience any of the above side effects on taking Amlodipine, report the same to your doctor immediately.
Before taking Amlodipine, you must inform your doctor about any medications, nutritional supplements, and herbal medicines you may be taking to avoid any drug interactions.
An interaction is when a substance changes or modifies the way a drug works. This may cause harmful effects or prevent the drug’s required effect.
Amlodipine interacts with a wide range of drug groups:
Taking diltiazem (another calcium channel blocker) with Amlodipine may increase the level of Amlodipine in the body and cause more side effects.
Taking antifungal medicines like ketoconazole, itraconazole, or voriconazole with Amlodipine may increase Amlodipine levels in the blood.
Taking clarithromycin with Amlodipine may increase Amlodipine in blood, increasing the risk for more side effects due to the medicine.
Taking medicines like sildenafil, tadalafil, avanafil, or vardenafil along with Amlodipine may increase your risk of low blood pressure.
Taking Amlodipine with simvastatin (a cholesterol-lowering drug) may result in higher levels of simvastatin in the blood.
This could result in more side effects due to the drug.
Taking Amlodipine with medications like cyclosporine and tacrolimus may result in higher levels of these medicines in the blood.
This can increase the risk of immune system-related side effects.
Other drugs that are known to show severe interactions with Amlodipine are:
Cytochrome P450 Family 3 Subfamily A Member 4 or the CYP3A4 gene is a member of the cytochrome P450 family.
The CYP genes participate in drug metabolism (chemical alteration of the drug in the body), production of cholesterol, steroids, and other lipids.
Amlodipine is metabolized in the liver by CYP3A4 and CYP3A5 genes.
Therefore, any changes in the activity of these genes can lead to a modified effect of Amlodipine.
A study published in JAMA (Dec 2018) states that coadministering Amlodipine and clarithromycin or erythromycin increases the risk of hypotension (low blood pressure) and acute kidney injury.
This effect is said to be due to decreased metabolism of the drug by the CYP3A4 enzyme.
Another study reports that CYP3A4 gene types partly determined blood pressure response to Amlodipine in high-risk African-American patients.
Natriuretic Peptide A or NPPA gene is a gene that belongs to the natriuretic peptide family.
This family of genes is responsible for maintaining salt and water balance in the body.
This gene is located on chromosome 1.
rs5065 (also called T2238C) is a single nucleotide polymorphism or SNP in the NPPA gene.
A study published in JAMA in 2009 stated that SNP rs5065 played a role in modifying the antihypertensive medication effects on blood pressure and the cardiovascular system.
According to the study, patients with the C allele showed favorable cardiovascular disease outcomes on taking diuretics.
In contrast, TT allele carriers showed promising cardiovascular results on taking calcium channel blockers like Amlodipine.
If you suffer from liver disease or heart valve problem (arterial stenosis), inform your doctor about the same before taking Amlodipine for hypertension.
If you are allergic to Amlodipine or experience a hypersensitivity reaction due to it, avoid taking the drug and report to your doctor immediately.
Studies conducted on animals show that taking Amlodipine during pregnancy may have adverse effects on the fetus.
Though there aren’t many human studies to determine how Amlodipine affects human pregnancy, it is best to inform your doctor if you are pregnant or planning a pregnancy while taking the drug.
Though limited, research states that Amlodipine may pass into breast milk and may cause side effects in a breastfed child.
If you are breastfeeding your child, inform your doctor about the same before taking Amlodipine.
As you age, your body’s ability to process Amlodipine reduces, making it stay in your body longer.
This increases the risk of side effects in older patients.
Genetic testing helps your doctor understand how your body may react to a particular drug.
It also helps your doctor determine the appropriate dosage of a drug for you.
For safe consumption of Amlodipine, you may need to get CYP3A4 gene testing done.
Gene testing may also be recommended if you need to take any other medication with Amlodipine, especially antibiotics like clarithromycin or erythromycin.
Analyze Your Genetic Response to Amlodipine
References:
With the beginning of the human genome mapping in 1990, there were hopes of finding the “gene for sports”. As it turned out, it wouldn’t be the most straight-forward thing ever. Athletic performance is not related to one factor only.
It is a complex system of interrelated intrinsic (genetics, physiological and psychological conditions) and extrinsic (training, and nutrition) factors. Some athletes seem to be gifted and have demonstrated extraordinarily high-performance levels.
Sports genetics is still a recent field of investigation. Due to its complexity, it is challenging to determine which genetic factors help increase or improve someone’s performance. By 2009, more than 200 genetic variations had been associated with physical performance and more than 20 variations associated with elite athlete status.
The most studied variations are related to the ACE and ACTN3 genes. The ACE (angiotensin-1 converting enzyme) gene codes for an enzyme that controls blood pressure. An ACE I/I genotype is related to endurance performance and higher exercise efficiency, while an ACE D/D genotype is associated with strength and power performances.
The ACTN3 gene codes for alpha actinin-3, a protein found in the fast-twitch muscle fibers used in explosive activities. These fibers provide quick bursts of strength. Many studies discovered that having the R allele of the ACTN3 gene, which produces the normal alpha actinin-3 protein, is common in athletes who rely on strength and speed. Sports that require rapid muscle contractions include boxing, baseball, and sprint races.
Another version of the ACTN3 gene (the R577X variant or the X allele) results in a complete absence of the alpha actinin-3 protein. It limits the proportion of fast-twitch muscle fibers and increases the proportion of slow-twitch fibers, without causing any diseases. Some studies found that this variation is more common in endurance athletes such as cyclists, cross-country skiers, and long-distance runners.
In the 2008 Olympics, Jamaica had the 4 fastest women sprinters in the 200 meters event. Interestingly, 98% of Jamaicans have the R variant of the ACTN3 gene. This variant produces the alpha actinin 3 protein that provides quick bursts of energy.
While some researchers focus on variations that increase performances, others are interested in genes related to injuries and the ability to recover from them. Tendinopathy is a common injury among athletes. It causes burning pain, and reduced flexibility. This tendon injury takes up to six months to heal. Polymorphism within COL5A1 and TNC genes has been associated with Achilles’ tendon injuries, which can be completely debilitating for some athletes. Also, variants in the MMP3 gene that plays a role in connective tissue wound repair can increase the risk of other tendinopathies.
Polymorphism within COL5A1 and TNC genes has been associated with Achilles’ tendon injuries, which can be completely debilitating for some athletes.
The frequency of genetic variations related to athletic performance differs across ethnic groups. For example, 25% of Asians, 18% of Caucasians, 11% of Ethiopians, and 2% of Jamaicans and US African Americans have the XX genotype of the ACTN3 gene. Jamaicans have an interestingly low frequency of XX genotype, which might explain why in the 2008 Olympics Jamaica had the four fastest women at the 200-meters sprint, four of the top six at 100 meters, and the fastest man at 100 meters.

A lot of athletes were lucky enough to have specific genetic variations that gifted them with what some people would call “superpowers”. One man who needs no introduction, the Jamaican Usain Bolt, finished his sprinter career with the title of the fastest man alive. Bolt won consecutive World Championships, from the 100 meters and 200 meters sprints, all the way to the 4 x 100-meter relay, bringing home more gold medals that one would care to count, spanning from 2009 to 2015. Imagine running 100 meters in 9.58 seconds. Insane, or should we say Usain, isn’t it? Unsurprisingly, Bolt is one of the 98% of Jamaicans with the ACTN3 R allele, giving him, to say the least, a considerable edge in feats of strength and speed.
Usain Bolt who set an incredible record of running 100 meters in 9.58 second has the ACTN3 R allele.
Another athlete worth mentioning is Eero Mantyranta, one of the most successful Finnish cross-country skiers to have walked - or skied- the earth. Mantyranta, who passed away in late 2013, had a rare genetic variation in the EPOR gene that made his body overproduce red blood cells. Red cells convey oxygen to the muscles; The equation from that point on is not exactly quantum physics: the more red blood cells one has, the happier the muscles, the longer they perform.
Skiing legend Eero Mantyranta was found to have a rare genetic variation in the EPOR gene that made his body overproduce red blood cells. This pushed more oxygen to his muscles, thereby increasing their efficiency.
To put it simply, you just don’t run out of gas as fast as your average Joe: You’re more endurant. That’s why some athletes dope themselves by injecting erythropoietin (EPO) into their systems, a hormone that stimulates red blood cell production. Mantyranta, with his EPOR variation, boasted a red blood cell concentration 50% higher than the average population. He took the golden medal for the 15km race home with an astonishing 40 second advance time on his closest competitor, an achievement never done before, and never accomplished by anyone else ever since.

And now, all the way from the snowy slopes to the depth of the swimming pool, an article on the role of genetics in sports wouldn’t see the light if Michael Phelps’s name wouldn’t appear in it somewhere! An American swimmer better known for having a total of 28 Olympic medals under his belt. Phelps is 6 feet 4 inches tall, however, he has the torso of a man 6 feet 8 inches tall and the legs of a man 8 inches shorter. His disproportionately large chest enables him to have a longer wingspan (the distance from fingertip to fingertip when the arms are stretched out to the sides) than your average human being. The longer your wingspan, the further you can reach, or in Phelps’s case, the further he can stroke.
Great swimmers have disproportionate arms length and wingspan compared to the average person. Michael Phelps' lower body is proportionate with that of someone of 5'5" height, while his upper body is proportionate with that of a 6'5"tall individual.
On top of that, Phelps has hyperextended joints which, paired with his size, enables him to use his legs like flippers, thrusting him through water. In addition to special body proportions, Phelps’ genetic profile also provides him with a lower-than-average lactic acid production. The body produces lactic acid in response to high-intensity activity, which makes you feel tired and sore. Michael the “Flying Fish” Phelps produces low levels of lactic acid, exponentially decreasing his recovery time. Between his genetic profile and his sheer will, Phelps is without doubt, an elite swimmer and one of the most successful athletes having swam the earth’s swimming pools.
Another athlete boasting lower-than-average lactic acid levels, and therefore having never (or almost never for what we know) experienced muscle cramps is Dean Karnazes, an American runner. This athlete has a rare genetic variation that allows his body to rapidly flush lactic acid from his system. Typically, as you exercise, the body converts glucose to energy which produces lactic acid as a by-product. As it builds up in the muscles, it begins causing cramps and fatigue as a signal to stop whatever physical effort you’re undertaking. However, Karnazes is lucky enough to never receive those signals, thus enabling him to keep running for long, long periods. This genetic variation allowed Karnazes to complete fifty marathons in fifty states in fifty days in 2006: that’s one marathon a day without recovery time or rest. He also took it an extra mile (miles actually) further by running non-stop for three days in a row.
Although athletic performance is a multifactorial trait determined by both genetic and environmental factors and their plethoric interplay, a genetic profile may serve as an additional tool assisting athletes and their coaches to choose a specific sport that best matches their talent. Despite seemingly similar metabolic characteristics of all power performances, it seems that different genetic makeup enables an athlete to excel in speed-oriented sports like sprints or in strength-oriented sports like weightlifting. The future of genetic studies involving athletes is promising. However, it’s a very long way until we figure out the exact role of genetics for each different sport and what are the variants (at the molecular level) accounting for better performances and their mechanism of action.
This inadvertently gives birth to a vast array of questions and issues: Do the suggested genes and their variants give similar advantages to different age groups such as kids and adolescents? Will genetic testing and gene screening be enough to predict performance or tailor workout training programs for athletes? Will gene manipulation become, along with doping, the newest threat to sports’ ethics? Will genetic manipulation one day take a toll on both the physical and mental health of athletes?