Osteoporosis, a bone disease affecting seniors and menopausal women is a growing concern causing over 8.9 million fractures each year worldwide (Johnell et al, 2006). In India, there are an estimated 25 million people who may be suffering from osteoporosis. Both men and women are affected with the disease at an earlier age compared to the West (Malthora and Mittal, 2008).
| Defining the Disease Osteoporosis is a disease of the bone where density progressively decreases over the years. Those who suffer from the condition are at high risk of falling and injuring themselves severely resulting in hip fractures. Worldwide, approximately 28-35% of people, over 65 years and above fall annually (Blake et al, Prudham, and Campbell et al) and the incidence rises to 32-42% in seniors over the age of 70 (Tinetti et al, Downton & Andrews, and Stalenhoef et al). |
|---|
| Is It Genetic? There are several causes of osteoporosis. Although certain factors such as age, medications and disease and lack of essential vitamins and mineral for bone development are at the forefront of why osteoporosis occurs, there is also the belief or theory that genetics play a role. In women, who are at a higher risk of contracting the disease especially at an older age, the prevalent threats include sedentary lifestyle, cigarette smoking and an excessive intake of alcohol. |
|---|
| Studies that Support Osteoporosis is Hereditary There are several studies and researches that point to the DNA makeup as one of the culprits when it comes to the bone disease. A senior person whose family history includes bone and hip fractures has a bigger risk of going through or suffering from the same condition. In addition, those with a small body structure and frail bones are at a higher risk of lower bone density even at an early age. Ralston in the study, ‘Genetic Determinants of Osteoporosis’ explained the genes and genetic variants that are linked to the condition and the management of bone mass. The research also identified the genetic markers in assessing fracture risks. Another study by Estrada et al identified 56 genetic variants (bone mineral density loci) and determined 14 loci are linked to fracture risks. It gave a better understanding of the genetic structure of bone mineral density and how it affects fracture susceptibility. Twin and family studies have also demonstrated that 50% to 85% of the differences in BMD is due to genetic variances (Peacock et al, 2002). |
|---|
| Race and Ethnicity Another factor is racial makeup, with Caucasians or Asians more likely to get osteoporosis than other ethnic groups. Cauley in her study, ‘Defining Ethnic and Racial Differences in Osteoporosis and Fragility Fractures’ revealed that race and ethnicity have some bearing on the incidence of fractures, with the highest rates recorded in white women. Among men, there is not much variance with other ethnic and racial groups, but the incidence of bone fracture is higher in white men than those of Asian or African descent. (Cummings et al, 2002). Hochberg in his study, ‘Racial Differences in Bone Strength’ affirms that fracture risk is higher among whites than blacks in the US. This was due to the greater bone strength (mass, porosity and composition as well as damage) among blacks compared to whites. Stronger bones in blacks are attributed to the development of a sturdier skeleton and lower bone loss during adulthood. |
|---|
| Management of Osteoporosis Osteoporosis is strongly linked to genetics, but its incidence can be prevented. Loss of bone density can be averted by consuming adequate amounts of calcium and vitamin D for stronger bones. Other methods include engaging in weight-bearing exercises, and avoiding certain drugs that affect bone loss. Women also have the option to start estrogen replacement therapy which can reduce bone density.Osteoporosis is a disease of the bone where density progressively decreases over the years. Those who suffer from the condition are at a high risk of falling and injuring themselves severely resulting in hip fractures. Worldwide, approximately 28-35% of people, 65 years and above, fall annually (Blake et al, Prudham, and Campbell et al) and the incidence rises to 32-42% in seniors over the age of 70 (Tinetti et al, Downton & Andrews, and Stalenhoef et al). |
|---|
The COL5A1 gene is associated with the synthesis of type V collagen, a key constituent of ligaments and tendons. Specific alleles of this gene are known to either increase or decrease the risk of injury.
| CHIP Version | COL5A1 SNPs |
| 23andMe (Use your 23andme raw data to know your COL5A1 Variant) | |
| v1 23andme | Present |
| v2 23andme | Present |
| v3 23andme | Present |
| v4 23andme | Present |
| V5 23andme (current chip) | Present |
| AncestryDNA (Use your ancestry DNA raw data to know your COL5A1 Variant) | |
| v1 ancestry DNA | Present |
| V2 ancestry DNA (current chip) | Present |
| Family Tree DNA (Use your FTDNA raw data to know your COL5A1 Variant) | |
| OmniExpress microarray chip | Present |
A study conducted on people with Achilles tendinopathy showed that those with the CC genotype of COL5A1 were associated with a lowered risk of developing Achilles tendinopathy compared to people with the T variant. Similar results were seen among people with anterior cruciate ligament injuries, again people with the CC genotype were found in lower numbers in a group of people with an ACL injury.
In terms of flexibility, people with the T variant of the gene are associated with a lower range of motion, implying that they could be less flexible. People with the TT genotype have tendons that are stiffer than those with the CC genotype. The stiff tendons and the lowered range of motion could be the reason behind the potential increase in the risk of injury among people with the TT genotype.
Stiffer Achilles tendons have an increased capacity to store and return energy thus providing an advantage in endurance running. This would mean that people with stiff Achilles tendons would require a lower amount of energy for every step, making such runners more efficient. This is what makes people with the T variant (less flexible) better suited for long-distance running events. Support for this theory comes from an ultra-marathon running study conducted in 2011. The study reported that people with the T variant had stiffer tendons but finished significantly faster than people with the C variant of the gene Col5A1.
In a study conducted on people with a self-reported history of exercise-associated muscle cramping, people with the C variant were shown to be over-represented among people with no history of exercise-associated muscle fatigue.
| Genotype | Phenotype | Recommendations |
| TT | [Limitation] More likely to have stiff tendons and increased risk of injuries and tendinopathies. [Limitation] Likely to have decreased range of motion (flexibility) [Advantage] Better endurance [Limitation] More likely to have a higher risk of muscle fatigue/ muscle cramping | Likely better at endurance running than the C variant Increased risk for injuries - warm-ups and stretching before workouts are important to avoid injury. Recuperative therapies such as massages can help |
| CT | [Limitation] More likely to have stiff tendons and increased risk of injuries and tendinopathies. [Limitation] Likely to have decreased range of motion (flexibility) [Advantage] Better endurance [Limitation] More likely to have a higher risk of muscle fatigue/ muscle cramping | Likely better at endurance running than the C variant Increased risk for injuries - warm-ups and stretching before workouts are important to avoid injury. Recuperative therapies such as massages can help |
| CC | [Advantage] More likely to have an increased range of motion (Flexibility) [Advantage] Lower risk of ACL injuries and Tendinopathies [Limitation] Lower endurance [Advantage] More likely to have a lower risk of muscle fatigue/ muscle cramping | Greater flexibility due to an increased range of motion allows you to perform a variety of different exercises easily. A lower risk of injury allows you to remain active and train often. |
“Nutrigenetics, fitness genetics, health genetics are all nascent but rapidly growing areas within human genetics. The information provided herein is based on preliminary scientific studies and it is to be read and understood in that context.”
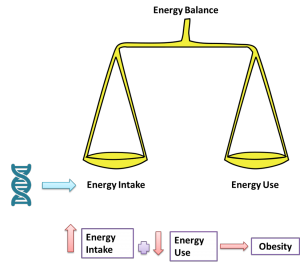
A healthy weight is maintained during a state of energy balance- when the energy intake of an individual matches the energy expenditure. Weight can accrue over a long period of time if the intake is higher than expenditure. Besides intake and expenditure, other factors such as age, basal metabolism, hormonal imbalance, and genetics also influence weight gain or weight loss.
Many humans have inherited genetic adaptations, which evolved to mitigate the ancestral exposure to cycles of feast and famine. Hence, the human body is very good at storing excess energy as fat and reluctant to lose valuable stores (fat) of energy. This is the basis of the ‘thrifty gene’ hypothesis, which explains why people easily put on weight on an excess calorie diet and find it very hard to lose it.
The heritability associated with energy intake among children is found to be between 47-69%. Twin studies showed that there was a genetic influence on the type of food consumed, along with satiety and food cue response.
There are many genes that have been shown to be associated with obesity and energy intake. Of particular significance is the FTO gene. Studies have shown that certain variants of this gene were associated with increased energy intake and increased hunger. Individuals with the abnormal FTO gene weigh at least 3kgs more than individuals who have the normal copy of the gene.
Individuals with an abnormal copy of the FTO gene eat more frequently, with a tendency to prefer calorie-dense foods and larger portions of food. People with the highest risk variant should exert portion control and eat a lot of food rich in fiber which would help quell the hunger. They should also consider frequent snacking in small quantities of low calorie, high protein, and high fiber foods to counteract the perpetual hunger they may be experiencing to maintain a stable glycemic index and stable levels of hunger and satiety hormones.
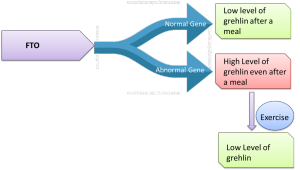
A hormone that plays a key role in satiety is ghrelin. Ghrelin is responsible for ‘hunger pangs’ as it signals the brain to eat. After a meal, the level of ghrelin is lowered and levels of another hormone, Leptin, are elevated resulting in a feeling of fullness. In an individual with the high risk variant of the FTO gene, the level of ghrelin remains high even after a meal, re
sulting in over eating. In such individuals, exercise has been shown to restore the level of ghrelin to normal levels.
Individuals with the abnormal FTO gene should be encouraged to follow a regular exercise pattern which will aid in lowering ghrelin levels and provide better satiety response.
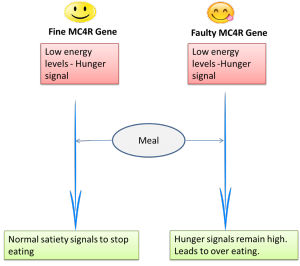
Another important gene that affects meal size and meal choice but not meal frequency is MC4R. When the energy levels drop in our body, the hunger center sends signals that inhibit MC4R and there is an increase in appetite. When the stomach is full after eating, satiety signals are sent by the satiety center that stimulates the MC4R to send signals to stop eating.
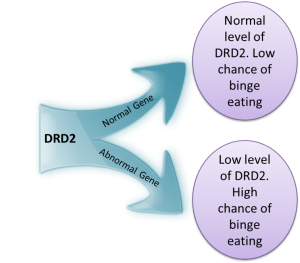
Overeating that is induced by distress, emotional eating, leads to binge eating which is highly prevalent in adults who are binge eaters or obese. Binge eating disorder is due to hypersensitivity to reward which results in overeating. The tendency to overeat or binge eat can be determined relatively strongly by analyzing the dopamine D2 receptor gene.
Dopamine is a neurotransmitter and its secretion is increased during emotional upheavals. From an evolutionary aspect, this hormone is released in response to some adverse condition, to prepare the body for a flight or fight response. Under normal circumstances, when dopamine binds to the DRD2 receptor, it should lower feelings of hunger and increase satiety. However, mutations in the DRD2 gene lead to a lower amount of DRD2 in the brain, which could lead to binge eating or overeating.
Individuals who carry the abnormal gene should consciously avoid overeating when feeling distressed or should store healthy snacks to eat at times of distress. Another study showed that deficits in the dopamine D2 receptor led mice to be inactive, which in turn lead to weight gain. Therefore, people with an abnormal gene should consciously stay active.
Regulating energy intake can moderate susceptibility to weight gain and obesity and is essential for people with a higher propensity to gain weight. Interventions that promote self-regulation of energy intake have the potential to control weight gain and also encourage healthy dietary habits. When designing intervention strategies, it is important to understand the genetic aspects involved as nearly 30% of obese individuals underreport their energy intake. The most effective way to fight obesity is through calorie restriction or lowering energy intake. People who carry abnormal genes for energy intake should follow mindful eating to ensure a balance in energy homeostasis.
Individuals who carry the abnormal gene should consciously avoid overeating when feeling distressed or should store healthy snacks to eat at times of distress. Another study showed that deficits in the dopamine D2 receptor led mice to be inactive, which in turn lead to weight gain. Therefore, people with an abnormal gene should consciously stay active.
Regulating energy intake can moderate susceptibility to weight gain and obesity and is essential for people with a higher propensity to gain weight. Interventions that promote self-regulation of energy intake have the potential to control weight gain and also encourage healthy dietary habits. When designing intervention strategies, it is important to understand the genetic aspects involved as nearly 30% of obese individuals underreport their energy intake. The most effective way to fight obesity is through calorie restriction or lowering energy intake. People who carry abnormal genes for energy intake should follow mindful eating to ensure a balance in energy homeostasis.
Find out which variations of these genes you carry and more at www.xcode.life
Nutrigenetics, fitness genetics, health genetics are all nascent but rapidly growing areas within human genetics. The information provided herein is to be read and understood in that context.
When opting for a healthy lifestyle, much of the difficulty we face is attributed to our diet. Why aren't we craving healthy foods? Why do some of us feel a surge of revulsion every time we see kale before us? It appears our food preferences run deeper, well into our genetic code.
Taste preference is a complex interplay of physiological, psychological, genetic and social factors of an individual. Among these, genes particularly play a significant role in influencing an individual’s taste and food preferences. By understanding the genes that play a role, it will help us align our diet based on our genes, and perhaps, this will help us eat healthier!
Of the 5 different senses we have, taste is the most personal of it all. It's uniquely ours, and is the determinant of what we choose to eat. Just as there are differences among humans in various physical traits due to genetics, there are myriad differences in taste preferences, sometimes major and often minor. Efforts have been underway since the early days to determine the origin of our taste preferences, and we now know they're genetically encoded.
Taste preferences are known to influence energy intake and there are many genes that are important in determining taste preferences, with the gene TAS2R38 being a significant one.
The TAS2R38 gene, short for Taste 2 Receptor Member 38, is located on chromosome 7 and is known as the 'bitter' gene. This gene encodes a receptor that may play a role in the perception of bitter taste. They also play a role in sensing the chemical composition of the gastrointestinal tract. Research shows that TAS2R38 gene influences 70% of the preference for bitter foods.
Studies on TAS2R38 began when some people found phenylthiocarbamide (PTC), a synthetic compound, bitter while other others had no taste for PTC. Since then, although many different forms of this gene have been identified, there are predominantly two forms - taster and non-taster. The taste was initially thought of to be an effect of natural selection, as identifying bitter taste would help in staving off toxic substances in the food. However, the non-taster variant is also quite popular in the general population and the notion of natural selection of taster variant was dropped. Recent studies reveal that demographic pressures largely influence this gene's expression
There are certain variants of TAS2R38 gene with an association to greater BMI. The three variants of the gene can result into classification of non-tasters, tasters and super -tasters. The non- tasters have high threshold and low sensitivity while tasters have low threshold and high sensitivity. The third category is the super tasters who have an increased sensitivity. The taste perception of these three variants differs considerably, for example non-tasters perceive scotch as less bitter and more sweet than super tasters.
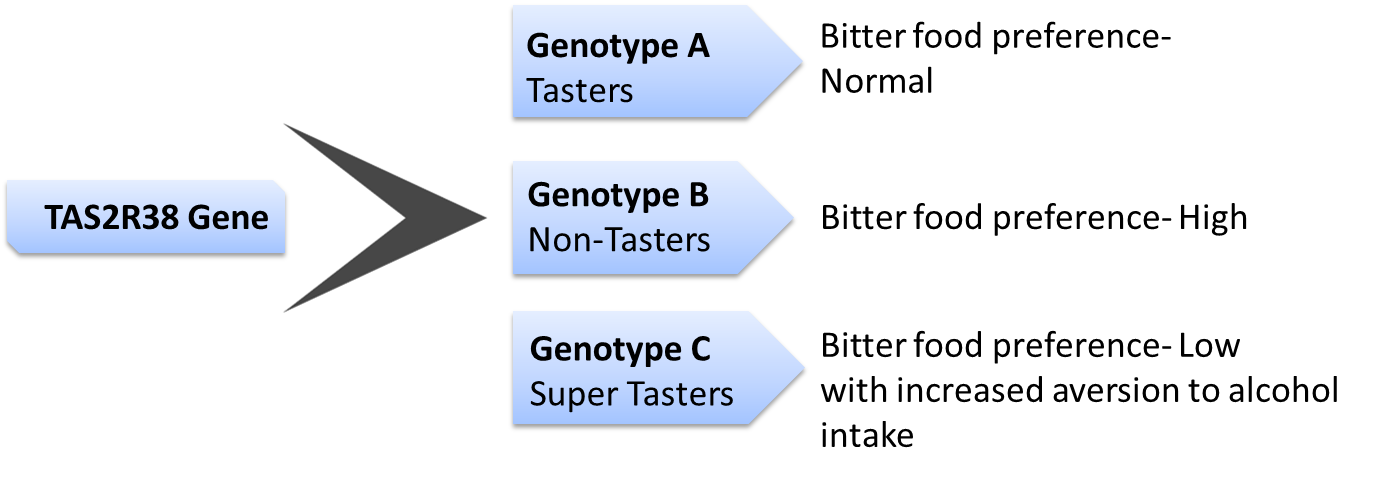
People with the non-taster version of the gene should modulate their energy intake to prevent excess intake of alcohol, or other high calorie bitter foods which can potentially increase their risk of obesity and other associated conditions.
Several genes influence our preference for sweet tastes. These include TAS1R1, TAS1R2. TAS1R3. The genes work interdependently. For example, the protein produced by TAS1R3 binds to the protein TAS1R1 to form a pleasant savoury taste, umami response or it could bind with TAS1R2 to form a sweet taste response.
The variants of TAS1R1 play an important role in food preferences. Apart from food preference, TAS1R2 is present in various parts of the body and could play a role in sugar metabolism, contributing to inter-individual difference in energy intake.
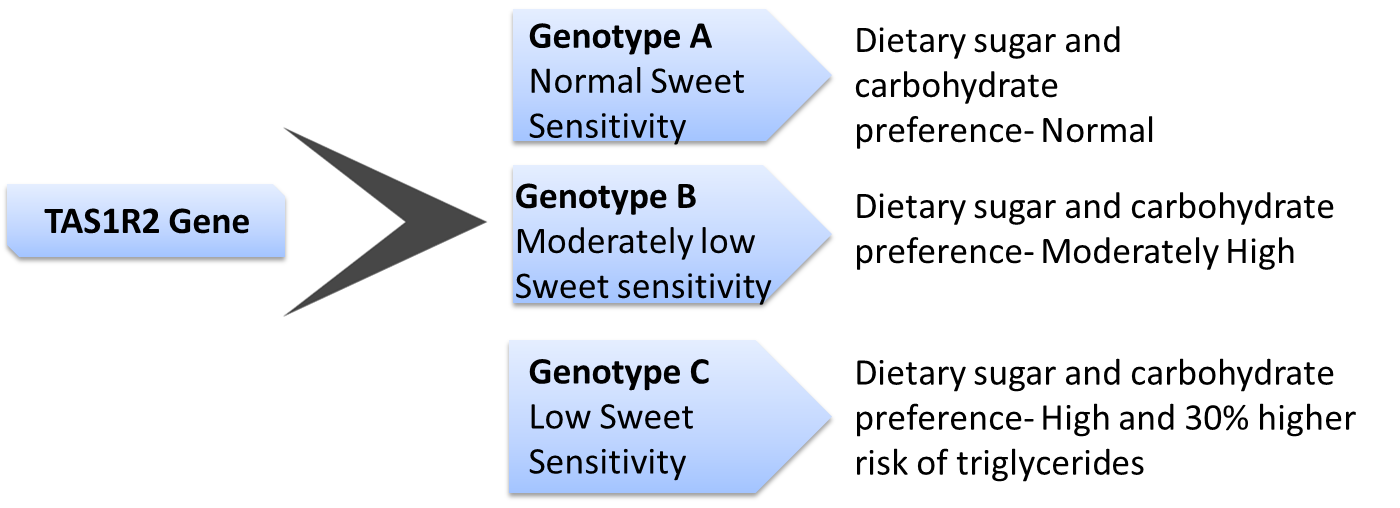
Individuals with the ‘high risk’ genotype can modulate the effect of the risk variant by controlling the amount of carbohydrate consumed.
An important food preference that can directly affect the risk for obesity is fat taste preference. Fat from dietary sources is not only essential for energy storage but is also vital for temperature regulation. An important gene that regulates our perception of taste of fatty food is the CD36. Located on chromosome 7, this gene influences the amount of fat consumed.
Having certain variants of CD36 gene can increase or decrease the levels of CD36 protein produced. For example, some variants produce low levels of CD36 are, therefore, less sensitive to fat with higher threshold for increased fat intake. On the other hand, individuals with high levels are more sensitive to fat in their diet, and hence consume less fat.
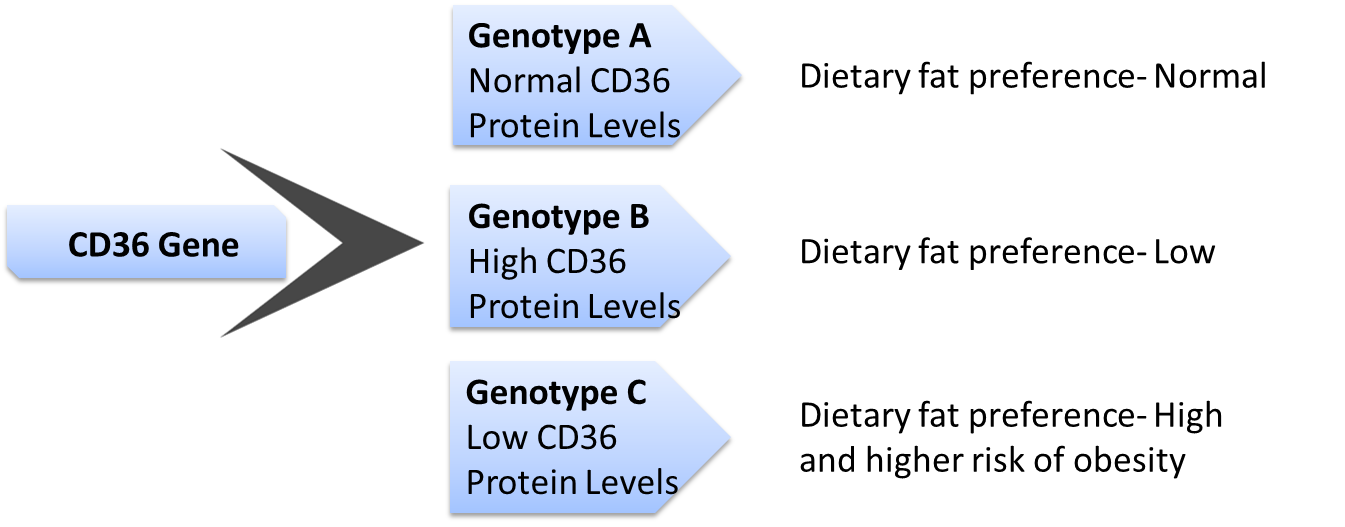
Individuals with a high preference for food rich in fat should modulate their risk for obesity by controlling fat content in their diet. Studies have also shown that such individuals could lower risk for cardiovascular disease and obesity by following a mediterranean diet.
The genetic variants that control our taste preference also have an association with obesity and other metabolic conditions. Metabolic syndrome is a combination of health issues that can increase our risk for certain serious health conditions like a cardiovascular disease or diabetes. Therefore, it has become all the more important to know the gene variants responsible for our food preference.
Taste is an individual preference, influenced by the genes that we carry, and dictating energy intake. An average human has over 9,000 taste buds and it is therefore no surprise that we love to eat! However, understanding the genes we carry will aid in making intelligent food choices for better health.
Want to know your genetics of taste preferences? Find out by uploading your DNA raw data to Xcode Life!
We are glad to learn about your interest in partnering with us. Please find below a list of frequent partnership queries that we receive.
➤ Which raw data is the best for getting the most from your reports?
We generate reports from pretty much any company which provides more than 5,00,000 genotypes. 23andme, FTDNA, ancestryDNA all provide this type of results. Please refer to the list below of raw data providers we accept data from. If your provider is not on the list, please send us a sample of raw data and we will let you know if its compatible with our process.
➤ Do you have a complete list of all the raw data providers compatible with your tool?
Please refer this link for a complete list of all raw data providers compatible with our tool: https://www.xcode.life/23andme-raw-data/ancestry-dna-raw-data-providers-for-xcode-health-reports
➤ Do you provide complete white labeling for reports and kits?
We brand the kits, reports and all other product related materials with your logo, provided an initial order of 100 units is placed.
➤ Do you provide API to present reports on my website?
We offer the results in JSON format so your applications can use the output on your website.
➤ Do you have a special pricing for partners?
We offer an average of 30% discount on the prices published on our website to our partners.
➤ Do you ship kits overseas?
Yes. We are able to ship kits internationally.
➤ How long does it take to produce results once the raw data is uploaded?
The reports will be ready in a few hours after uploading data.
➤ Do you customize the report as per my design and formatting requirements?
Yes we customize reports. There is one time USD 2500 customization charge applicable.
➤ Can you create custom reports on topics not currently listed on your site for my practice?
Yes we create special reports on various niche topics. Please write to us about your requirement.
➤ Do you offer exclusive distributorship in my country/territory?
Exclusivity of distributorship in your territory of business is available based on an upfront volume commitment.
➤ How long does it take for me to start working with your company?
You can be up and running in less than a week once the agreement is signed between us.
➤ Is there a minimum order requirement for partners?
There is no minimum order requirement for partners.
➤ What are the current products in your portfolio?
Please check this link for the list of all our products: https://www.xcode.life/product/ftdna-ancestrydna-23andme-raw-data-interpretation-analysis-tools/
➤ Do you provide reports in other languages?
We currently have reports in the English language. However, we can work with you in creating a version of the report in the language of your preference.
➤ Will you perform the laboratory protocols on the samples or is it better for us to find a local laboratory?
We can facilitate testing through our lab partners. However, it’s preferable to find a local laboratory in your country to do the testing and send us the raw data file for report generation. We can connect you with lab partners if need be.
Please feel free to drop an email to hello@xcode.life, if you are looking to take this forward, with your time preference. A call can be scheduled with the CEO/Chief Of Staff.
Look forward to partnering with you.
Also Read: Worrier Or Warrior? Analyze Your DNA Raw Data For COMT – The Warrior Gene
Weight loss struggles are an increasing phenomenon world over with the majority of people aspiring to achieve a slim body either for aesthetic reasons or good health. However, in recent years, obesity has increased dramatically in many parts of the world with India ranking third in the world’s most obese countries. According to a study, ‘Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013:a systematic analysis for the Global Burden of Disease Study 2013’, India accounts for 15% of the world’s obese population along with China.
With the rise in obesity, there has also been a significant rise in metabolic diseases associated with obesity such as diabetes, hypertension and heart disease. India has been particularly hard hit with rates of diabetes reaching as much as 20% of the population in some parts of the country. Even though accounting for only 20% of the world’s population, India shoulders 60% world heart disease burden. Studies claim that 40% - 70% of obesity is influenced by genetic predisposition, with environmental elements accounting for the rest. As alarming as this is, there is hope for change. Several scientific studies indicate that the prevention of metabolic conditions by lifestyle modifications such as healthy diet and exercise are far more effective than clinical treatment for these conditions at a later stage.
| With over 50% of obesity being attributed to genetics, obesity can be an inherited condition. Studies find that the risk for obesity is 2-8 times higher for a person with a family history as opposed to a person with no family history of obesity. The FTO gene, also commonly known as the obese gene, is considered to be highly contributory to obesity in individuals. People carrying this gene are found to have a 70% higher chance of being obese than non-carriers. Other genes such as MC4R, INSIG, TCF7L2, LEP, IRS, have also been found to contribute to this condition. However, this does not necessitate a certainty of obesity in carriers. Studies have found that corrective lifestyle measures can alleviate obesity even in people with a genetic predisposition. |
Apart from genetics, a variety of environmental factors have also contributed to this rapid increase in obesity. The most prominent of them being unhealthy food choices and decreased physical activity. The increase in access to junk and processed food has led to unhealthy snacking and food habits. Home-cooked meals are maybe visited once a day with the remaining meals consisting of take-outs or packaged food. In addition, a sedentary lifestyle with minimum to nil physical activity greatly adds to the rise of this condition. Another factor for concern is the lack of regular sleep patterns. Working night shifts and staying up late hours in the night have also shown to contribute to an increasing waistline.
Weight management through standard diets or weight loss plan is a key strategy to reduce the risk or more effectively manage metabolic diseases.
However, the vast majority of weight loss solutions either do not work or work temporarily as they are not sustainable over the long term. The global weight loss industry is estimated to be around USD 600 billion. However, a recent 10-year study by King’s College London determined that an overwhelming 99% of people attempting to lose or maintain weight loss will fail in the long run, indicating that the vast majority of the money spent on weight loss treatments is wasted.
A key reason for failure is a one size fits all approach. Diet plans are standardised on a few core ideas such as high protein, high fats or low carbs, and are extended to as many customers as possible to maximise the market reach. Here, it is assumed that everyone’s body is the same on the inside and hence the same recommendations should work for all. This assumption turns out to be misguided. Genetics impacts all aspects of our lives including how we metabolize foods. Some people are capable of eating all they can and are able burn off the calories, while some people struggle to manage their desired weight despite their best attempts. This is because the underlying genetics is different for all individuals. So far, the tools to understand an individual’s genetics were unavailable. However, over the last decade, with significant advancements in science and technology, these tools are now both available and affordable.
Handpicked article for you: Is Dr. Rhonda Patrick Diet For You? Analyze Your DNA Raw Data To Find Out Your Nutritional Needs!
In a recent study by Stanford University, people who followed a diet program tailored to their genetics were shown to lose as much as 2.5 times the amount of weight compared to people who followed a “standard” diet advice. Understanding one’s genetic profile can help individuals understand their body type and tailor their diets to foods best suited to them. A healthcare professional can use insights from the genetic test to then create a personalized diet to help individuals optimize their metabolism, and achieve their weight objectives, while reducing associated health risks.
Weight loss doesn’t just make one look and feel good, but greatly improves the day-to-day quality of life too. Energy levels, mood, temperament, immune system – all get a boost while reducing the risks for several health and metabolic conditions. In fact, healthy lifestyle choices have also found to help control certain conditions like Type 2 diabetes, PCOS and other lifestyle diseases. Not just for the obese or sedentary, proactive individuals should also consider undergoing a genetic test to understand their body’s unique metabolic profile to customise weight management program as per their lifestyle and genetics.
However, it is important to note that genetic testing can guide your effort correctly, but not replace it. Focussing on the overall nature of sustainable weight loss, Dr. M. Lakdawalla of CODS (Centre for Obesity and Digestive Surgery) India, says, “While genes do play some role in causing a predisposition to obesity, I would not say that they are entirely to blame. A paper published by Harvard's TH Chan School of Public Health states that ‘Active adults who carried the obesity-promoting gene had a 30 percent lower risk of obesity than inactive adults who carried the gene’. Worldwide, we have seen an increase in obesity over the past 30 years - it cannot entirely be put down to genetics. There are several factors that play a role - unhealthy lifestyles, rising stress levels, physical inactivity, rise in conditions such as diabetes, etc.”
Genetics is not just about physical differences among individuals. IT influences all aspects of human physiology and impacts several aspects of our health including, how our body responds to fats, carbohydrates, proteins, gluten, lactose, salt, and vitamins. This understanding will continue to grow by leaps and bounds in the years ahead. One thing is for certain, that the era of "standard" diets, nutrition, and medication is over. Evidence from several scientific studies indicates that what we consume as food and medicine need to be tailored to the individual's genetic type.