Estimated reading time: 13 minutes
Key Takeaways
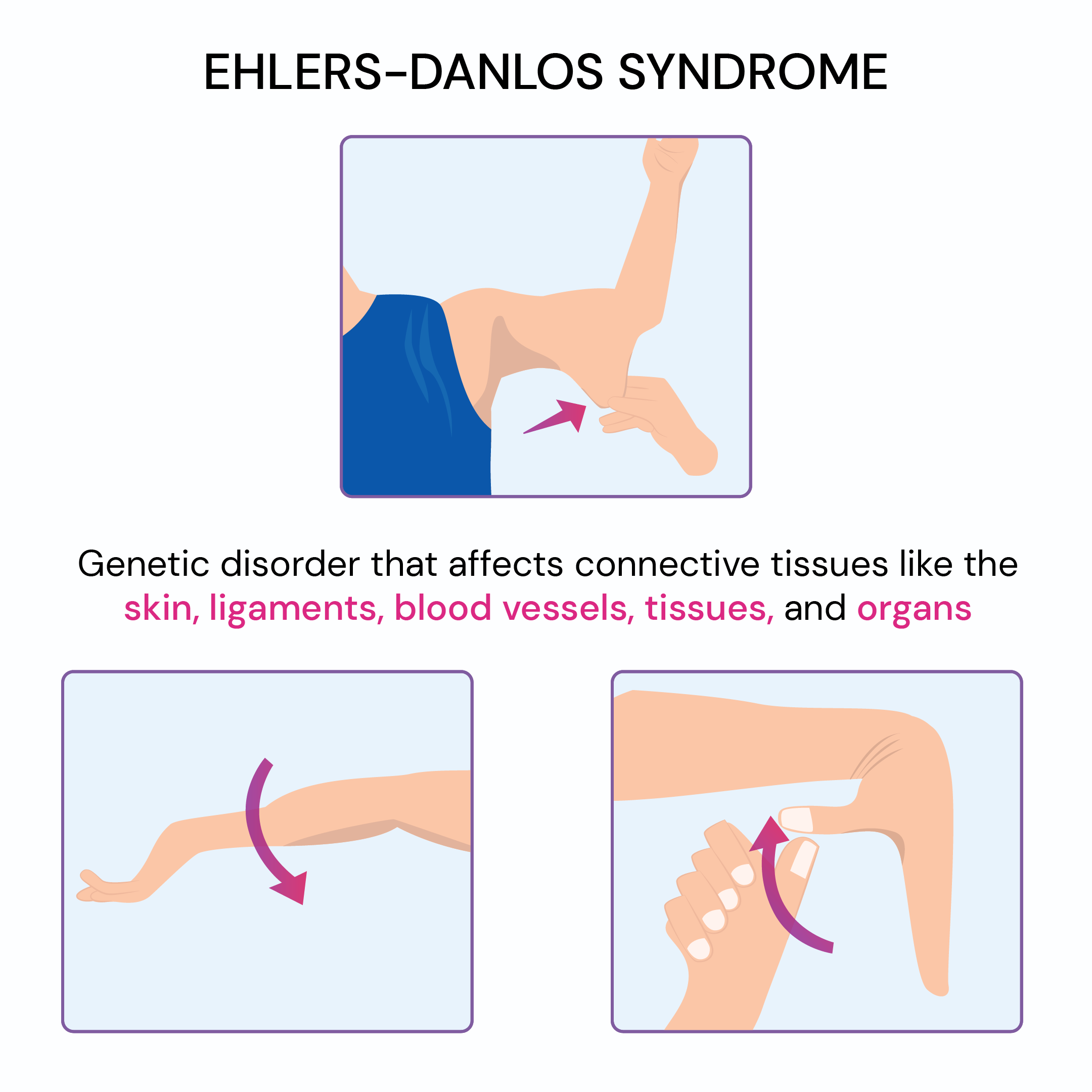
- Ehlers-Danlos syndrome (EDS) is a group of 13 genetic connective tissue disorders that affect the joints, skin, blood vessels, and internal organs.
- The most recognizable childhood signs of EDS include double-jointed flexibility, frequent joint dislocations, easy bruising, stretchy or soft skin, and slow wound healing.
- Many people with EDS also grow up with chronic fatigue, dizziness on standing, frequent headaches, and digestive issues, signs that reflect the nervous system and gut being affected, not just the joints.
- These signs tend to overlap with other conditions like fibromyalgia, hypermobility spectrum disorder, and even anxiety, making an accurate diagnosis challenging without clinical evaluation.
- While EDS has no cure, early recognition, lifestyle support, and personalized medical care can greatly improve quality of life.
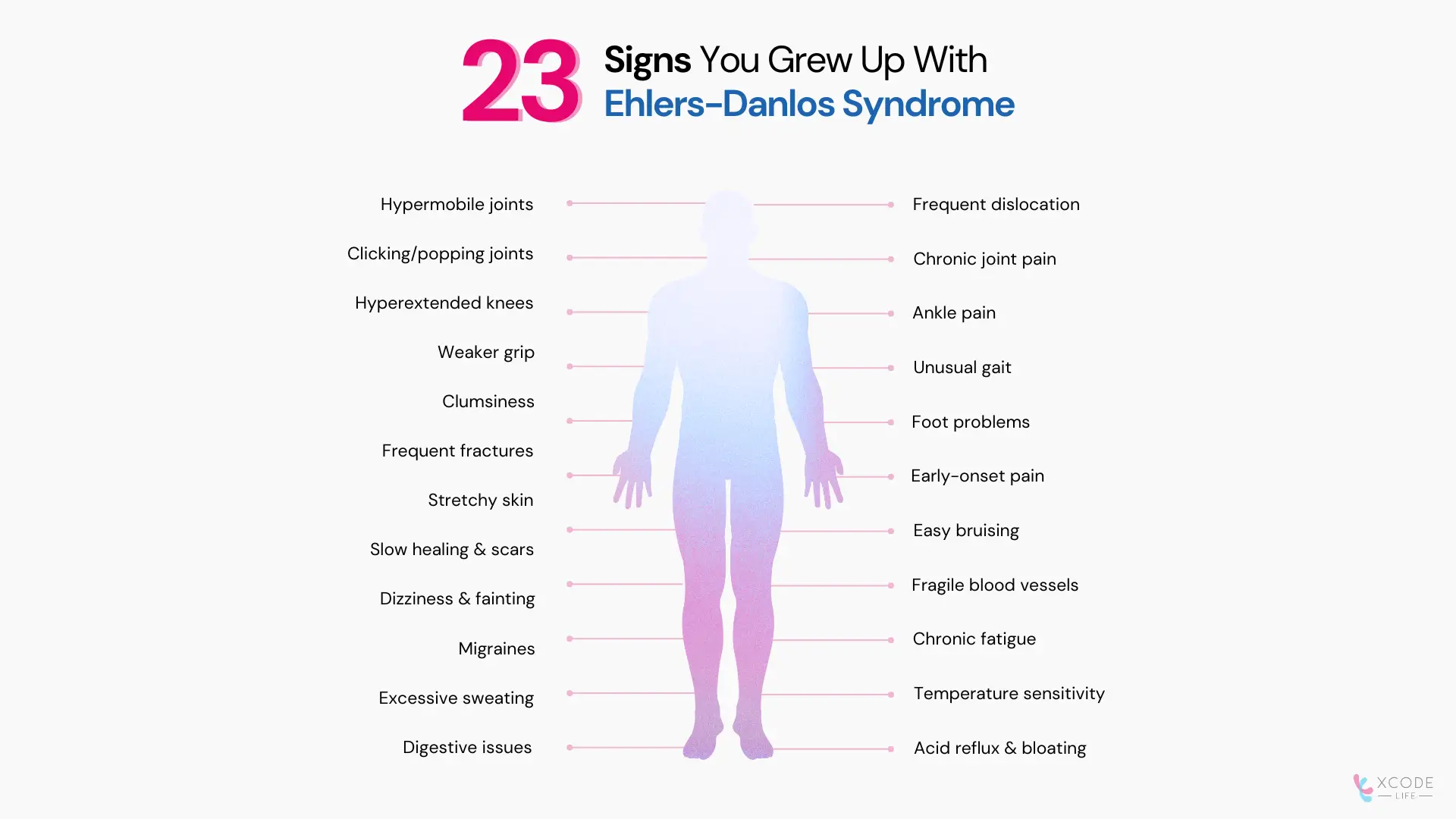
23 Signs You Grew Up With Ehlers-Danlos Syndrome
Joint & Musculoskeletal Symptoms
1. Hypermobile joints (double-jointed flexibility)
2. Frequent joint dislocations or subluxations
3. Clicking or popping joints
4. Chronic joint pain and instability
5. Hyperextended knees
6. Ankle pain during growth spurts
7. Weak grip strength (e.g., difficulty opening jars)
8. Clumsiness and uncoordinated movements
9. Frequent foot problems (flat feet, plantar fasciitis)
11. Chronic pain beginning at a young age
Skin & Wound Healing Issues
12. Soft, stretchy, or velvety skin
13. Easy bruising, often from minor contact
14. Slow wound healing and prominent or "cigarette paper" scars
15. Fragile blood vessels; prone to injury even under light pressure
Nervous System & Autonomic Symptoms
17. Dizziness and fainting, often linked to POTS (postural orthostatic tachycardia syndrome) [1]
18. Chronic fatigue
19. Frequent migraines or chronic headaches
20. Sensitivity to temperature changes
Digestive & Other Symptoms
21. Acid reflux and bloating
22. Nausea, constipation, or diarrhea (often linked to gastrointestinal dysmotility)
23. Bladder issues (urinary urgency or incontinence)
Note on Sign #23: Bladder and pelvic floor dysfunction are now recognized as common but frequently overlooked features of EDS, particularly in hypermobile EDS. Weak connective tissue in the pelvic floor contributes to these issues [2].
Common Signs Of EDS And Their Causes
| Sign | Likely Cause | Notes |
| Hypermobile joints | Weak connective tissue | Core diagnostic sign across subtypes |
| Easy bruising | Fragile blood vessels | Appears even with minor trauma |
| Slow wound healing | Collagen defects | May leave "cigarette paper" scars |
| Dizziness/fainting | Autonomic dysfunction (POTS) | Common in hypermobile EDS |
| Digestive issues | Weak connective tissue in gut | Acid reflux, constipation, bloating |
| Chronic headaches | Dysautonomia, TMJ dysfunction, craniocervical instability | Can also reflect Chiari I malformation [3] |
| Bladder symptoms | Pelvic floor connective tissue weakness | Underdiagnosed; seen especially in women with hEDS [2] |
What Do Experts Say About EDS?
Dr. Blair Grubb, a cardiologist specializing in autonomic disorders at the University of Toledo Health
Sciences, highlights the systemic nature of EDS:
- Hypermobility as a key diagnostic sign
- Cognitive issues in some patients ("brain fog")
- Abnormal autonomic test results** seen in a high proportion of patients with asymptomatic hypermobility*
- Higher rates of autism spectrum conditions in EDS patients
Research confirms this systemic view. A 2025 genome-wide association study (GWAS) meta-analysis of hEDS identified genetic correlations with myalgic encephalomyelitis/chronic fatigue syndrome, fibromyalgia, depression, anxiety, and autism spectrum disorder, confirming that EDS is fundamentally a multi-system condition [4].
*Asymptomatic hypermobility: A condition where a person's joints can move more than usual (are extra flexible), but they don't experience any pain or problems because of it.
**Autonomic test results: The outcomes from medical tests that check how well the body's automatic systems, like heart rate, blood pressure, and digestion, work.
Types of Ehlers-Danlos Syndrome
There are 13 recognized subtypes of EDS [5], ranging from common to ultra-rare. Some of the main ones include:
- Hypermobile EDS (hEDS): The most common subtype, estimated to affect approximately 1 in 500 to 1 in 5,000 people, and possibly more due to widespread underdiagnosis. Marked by joint instability, chronic pain, dysautonomia, and gastrointestinal involvement. Its precise genetic cause remained unknown for decades (see section below on the 2024 breakthrough).
- Classical EDS (cEDS): Caused by variants in COL5A1 or COL5A2 genes, leading to stretchy skin, poor wound healing, and prominent scarring. Prevalence is approximately 1 in 20,000 - 40,000.
- Vascular EDS (vEDS): Caused by COL3A1 mutations; it affects blood vessels and internal organs, carrying serious and potentially life-threatening risks. Prevalence is approximately 1 in 100,000- 200,000.
- Kyphoscoliotic EDS: Rare; marked by severe spine curvature from infancy and progressive muscle weakness.
- Classical-like EDS: Caused by TNXB mutations; similar to classical EDS but without the scarring pattern.
Important update on prevalence: The traditional figure of "1 in 5,000 for all EDS" is increasingly recognized as an underestimate when subtypes are considered individually. The Ehlers-Danlos Society now emphasizes that hEDS may be far more common than 1 in 5,000 and that a single combined prevalence figure masks the dramatic variation across subtypes [6].
Is Ehlers-Danlos Syndrome Genetic?
Yes, EDS is caused by variants in genes that produce collagen or the proteins that support connective tissue structure [7].
| Gene | Associated EDS Type | Function |
| COL5A1/COL5A2 | Classical EDS | Collagen type V production |
| COL3A1 | Vascular EDS | Collagen type Ill production |
| COLIA1/COLIA2 | Classical and rare types | Collagen type I production |
| TNXB | Classical-like EDS | Tenascin-X protein (supports connective tissue structure) |
| PLOD1 | Kyphoscoliotic EDS | Collagen crosslinking enzyme |
| KLK15 | Hypermobile EDS (some cases) | Kallikrein-15 protease; connective tissue and immune regulation |
| Expert picks: What To Read Next |
|---|
| Ehlers Danlos Syndrome And The Eyes |
| Which Parent Carries The Autism Gene? |
2024 Breakthrough: Genetic Cause Of hEDS Identified
For many years, hEDS was the only EDS subtype without a known genetic cause. This made diagnosis rely entirely on clinical criteria and left patients without genetic confirmation of their conditions.
In June 2024, researchers from the Norris Lab at the Medical University of South Carolina published a landmark study identifying variants in the Kallikrein gene family, specifically a missense variant in KLK15 (p.Gly226Asp), as a likely cause of hEDS in some patients[8].
Key findings:
- In two multi-generational families studied, every member with hEDS carried the KLK15 p.Gly226Asp variant, while unaffected family members did not.
- Among 197 unrelated hEDS patients studied by whole-exome sequencing, 32.8% (65 patients) carried at least one rare variant in a KLK family gene.
- Genetically engineered mice with the equivalent KLK15 mutation showed connective tissue problems resembling hEDS, including weaker tendons and heart valve abnormalities, confirming biological plausibility.
- The KLK15 gene is expressed in many tissues affected by hEDS, and KLK15 protein interacts with at least 10 extracellular matrix proteins, the body's structural scaffolding.
A separate 2025 GWAS meta-analysis (1,815 hEDS cases, 5,008 controls) identified two genome-wide significant loci, including a regulatory region near the ACKR3 gene (atypical chemokine receptor 3), implicating neuroimmune and pain signaling pathways in hEDS pathogenesis [4].
Already tested your DNA? Here’s how to use it further.
If you’ve tested with Ancestry, 23andMe, or similar services, your raw DNA file can be analyzed for deeper health insights.
How Is Ehlers-Danlos Syndrome Diagnosed?
- Clinical exam: Beighton score (≥5/9 in adults) for hypermobility; assessment of skin extensibility, scarring, and family history [10].
- Family history: Many forms follow autosomal dominant inheritance.
- Genetic testing: Available for classical, vascular, and most rare subtypes, but not yet available for hEDS, which remains a clinical diagnosis.
- Differentiation: EDS is distinct from Marfan syndrome (tall stature, heart risks) and fibromyalgia (chronic pain without tissue fragility). A 2024 study highlighted ongoing misdiagnosis, with hEDS patients experiencing an average diagnostic odyssey of several years before a correct diagnosis [11].
The Diagnosis Conundrum: EDS vs. Marfan vs. Fibromyalgia
EDS, Marfan syndrome, fibromyalgia, and joint hypermobility syndrome share overlapping symptoms, including joint hypermobility and chronic pain.
- EDS is specifically marked by tissue fragility, skin hyperextensibility, and frequent dislocations.
- Marfann syndrome typically includes tall stature, long limbs, and cardiovascular issues.
- Fibromyalgia involves widespread pain without the structural connective tissue abnormalities of EDS.
The 2017 international EDS classification also introduced a distinct category, Hypermobility Spectrum Disorder (HSD), for those who have symptomatic joint hypermobility but don't fully meet hEDS criteria. The boundary between hEDS and HSD remains clinically debated [12].
Accurate diagnosis requires detailed clinical evaluation and, where applicable, genetic testing.
What Are the Treatments for Ehlers-Danlos Syndrome?
There is currently no cure for EDS, but treatment helps manage symptoms and limit complications [13].
Therapies & Rehabilitation
- Physical therapy improves joint stability and helps prevent dislocations. Resistance training to strengthen muscles around hypermobile joints is a cornerstone of management.
- Occupational therapy can make daily activities safer and easier.
- Braces and supportive devices may be recommended for weak joints.
Medications & Medical Care
- Pain relief with over-the-counter or prescribed medications (including low-dose naltrexone, which has emerging evidence in EDS-related pain) [13].
- Celiprolol (a cardioselective beta-blocker) is the only medication with clinical trial evidence for
- vascular EDS, reducing arterial events by up to threefold. It is used in Europe and is under evaluation in the United States [14].
- Blood pressure management is important in vascular types.
- Surgery may be considered for severe joint damage or organ complications, though healing is challenging in EDS.
Counseling & Genetic Guidance
- Psychological support for coping with chronic pain and lifestyle changes.
- Genetic counseling to discuss family planning and inherited risks.
Lifestyle Adjustments
- Low-impact activities, such as cycling, swimming, Pilates, and tai chi, are preferred over contact sports or heavy lifting, which risk joint injury.
- Mindfulness, relaxation techniques, and stress management can improve quality of life.
- Supportive footwear and ergonomic seating help protect joints.
- Sleep positioning aids such as body pillows or firm mattresses may improve comfort.
- A balanced diet rich in anti-inflammatory foods, adequate protein, and nutrients such as vitamin D, vitamin C (essential for collagen synthesis), B12, and iron may help, though dietary interventions should be personalized and medically supervised.
Holistic Approach to EDS Management
Diet and Supplements
- Anti-inflammatory foods: Prioritize whole foods such as leafy greens, antioxidant-rich fruits, and omega-3 sources (salmon, walnuts, flaxseed) to reduce systemic inflammation.
- Vitamin C: Often overlooked, vitamin C is a cofactor required for collagen synthesis. Some EDS specialists recommend ensuring adequate intake, though supplementation should be discussed with a physician.
- Nutrient support: Address common deficiencies in vitamin D (bone health and immune function), B12 (cognitive function), and iron (fatigue) through diet or supplements under medical guidance.
- Gut health: Include prebiotic foods (garlic, bananas, and oats) and probiotics (yogurt and kefir) to support gastrointestinal function, which is frequently impaired in EDS [15].
- Individualization: Tailor diets to comorbidities, for example, gluten-free for confirmed celiac disease or low-FODMAP for IBS symptoms.
Environment
- Ergonomics: Use supportive seating, joint braces, and adaptive tools to minimize strain on hypermobile joints.
- Sensory considerations: Mast cell activation syndrome (MCAS), common in EDS, can cause reactivity to allergens, fragrances, and environmental chemicals. Air purifiers and allergen reduction can help.
- Compression garments: May improve blood flow and reduce POTS-related dizziness and fatigue.
Exercise and Mindfulness
- Low-impact exercise: Swimming, Pilates, resistance training, and tai chi strengthen muscles without stressing fragile joints.
- Avoid high-impact activities that stress joints (running on hard surfaces, contact sports, gymnastics).
- Timing: Avoid vigorous exercise immediately after meals to minimize autonomic dysfunction flare-ups.
- Stress reduction: Meditation and breathing exercises can reduce anxiety and help manage chronic pain.
- Cognitive-behavioral strategies: CBT addresses the emotional toll of living with a chronic, fluctuating condition.
These strategies may work better for some individuals than others. Always consult a qualified healthcare professional before starting any new supplement or exercise program.
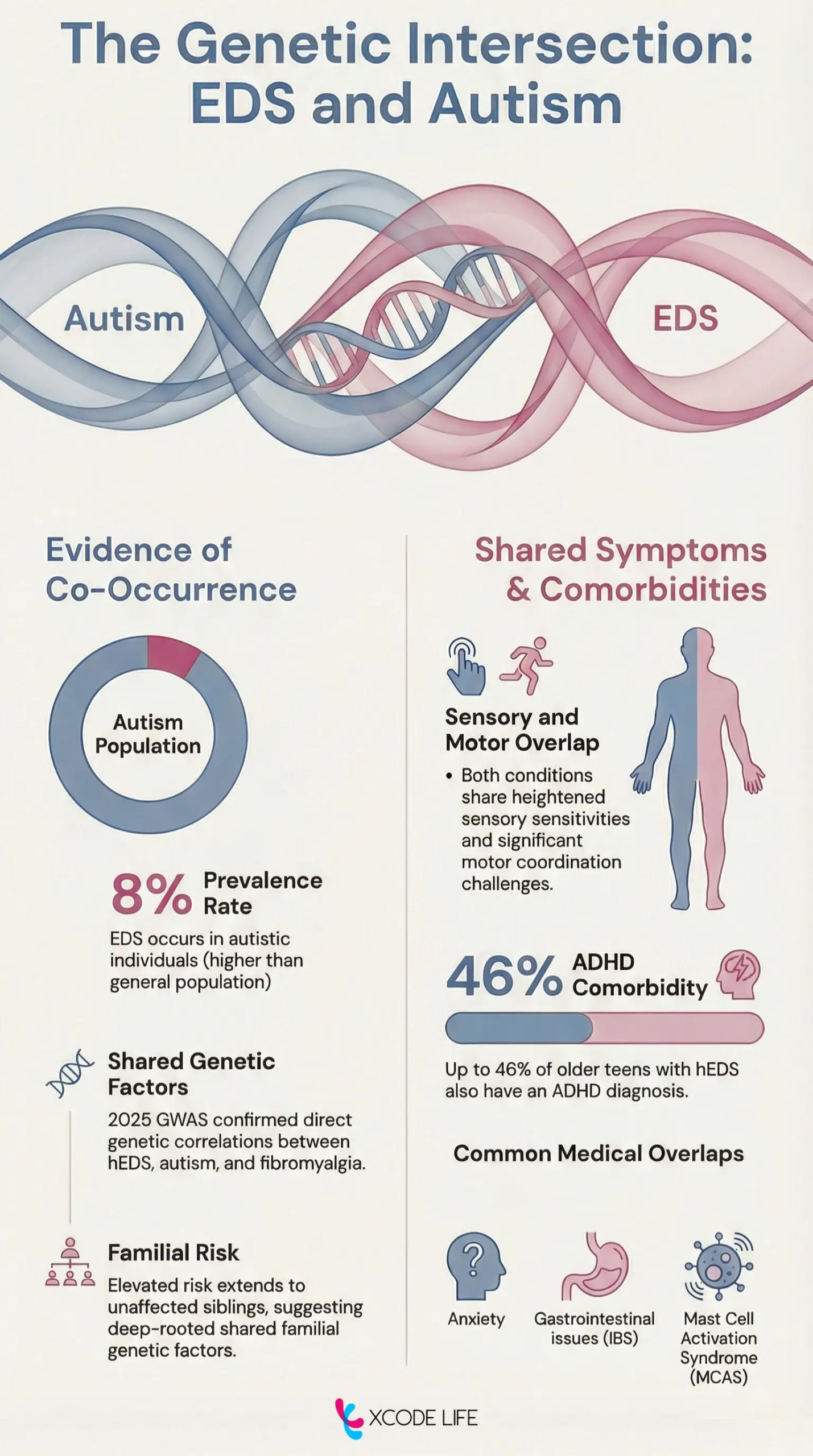
Can EDS And Autism Co-occur?
Yes, research suggests there are overlapping genetic factors and comorbidities.
Shared features include sensory sensitivities, digestive problems, and coordination issues.
ADHD, anxiety, fibromyalgia, and mast cell activation syndrome (MCAS) are also reported in both conditions.
Overlapping Symptoms
Symptomatically, both conditions share features such as:
- Sensory sensitivities: Individuals with EDS and autism often experience heightened sensitivity to light, sound, or touch.
- Motor coordination challenges: Joint hypermobility in EDS can lead to proprioceptive issues**, similar to motor difficulties seen in autism.
- Gastrointestinal problems: Digestive issues like irritable bowel syndrome are common in both conditions
**Proprioception is also called kinesthesia. It is the body's awareness of its position and movement in space, which is crucial for coordination and balance.
Overlapping Comorbidities
- ADHD: Attention-deficit/hyperactivity disorder (ADHD) is frequently reported alongside both EDS and autism. Shared neurological pathways may explain this overlap.
- Anxiety: Anxiety is common in both groups. In EDS, it’s often linked to chronic pain or autonomic dysfunction. In autism, it can stem from sensory overload or social stress.
- Fibromyalgia: Chronic pain and fatigue in fibromyalgia mimic symptoms in EDS and autism, making diagnosis tricky. These conditions all involve heightened sensory sensitivity and nervous system dysregulation.
Mast Cell Activation Syndrome (MCAS): MCAS, more common in EDS, can cause flushing, GI issues, and chemical sensitivities. Some researchers are exploring whether similar immune responses occur in autism too.
FAQs On Signs Of Ehlers-Danlos Syndrome
Beyond hypermobile joints and stretchy skin, EDS can produce less-recognized symptoms, including chronic headaches (from craniocervical instability), bladder urgency, "brain fog" and cognitive difficulties, temperature dysregulation, and heightened sensitivity to medications or anesthesia. POTS-related dizziness and mast cell reactivity are also widely reported but often overlooked in diagnosis.
For most subtypes, including the most common hypermobile EDS, life expectancy is not shortened when symptoms are well-managed [20]. The exception is vascular EDS, where the median survival is approximately 51 years due to risks of arterial rupture and organ perforation, though outcomes are improving with celiprolol therapy and earlier diagnosis [21].
Yes. Flexibility may paradoxically decrease over time (as joints become more damaged), while chronic pain, fatigue, and joint instability often worsen. Connective tissue weakness can accumulate through repeated microtraumas, dislocations, and injuries over the years.
Key red flags that should prompt clinical evaluation include unusually flexible joints from childhood, a family history of similar symptoms, delayed wound healing, wide or "cigarette paper" scars, recurrent joint dislocations, and unexplained chronic pain or fatigue. In vascular EDS specifically, a family history of early-onset arterial rupture or organ perforation is a critical red flag requiring urgent genetic testing.
Yes, EDS can indirectly affect hair. Altered collagen and skin structure in EDS can lead to enlarged or disrupted hair follicles, which may affect hair quality and texture. Some patients report thinning brittle hair, which may also be linked to nutritional deficiencies common in EDS (such as iron, B12, or vitamin D) [22].
Certain features are more common in specific subtypes. In vascular EDS, affected individuals may have thin, translucent skin, a narrow or thin nose, a thin upper lip, small earlobes, and prominent eyes. Those with fair skin tone ay have prominently visible blood vessels [13]. In some rarer subtypes, structural features such as a high-arched palate, dental crowding, and small chin may be present.
Yes. Fragile connective tissue can make breast tissue more prone to pain, strain, or injury, particularly with changes in weight or posture. Ligamentous laxity around the chest can also contribute to musculoskeletal chest pain, which is commonly reported in hEDS.
EDS is frequently confused with Marfan syndrome, Loeys-Dietz syndrome, fibromyalgia, joint hypermobility syndrome/HSD, chronic fatigue syndrome, and even anxiety disorders. The average diagnostic delay for hEDS is several years to over a decade, in part because many clinicians are unfamiliar with the condition's systemic features [11].
Some individuals with EDS appear younger than their age due to soft, elastic skin, a reflection of altered collagen structure. However, the same collagen fragility that makes skin smooth also leads to easy bruising, scarring, and tissue damage over time.
Yes. EDS is a lifelong condition. Chronic pain is reported in approximately 90% of patients with hypermobile EDS [23], and management is centered on symptom control, joint protection, and quality of life rather than a cure.
Summary: 23 Signs You Grew Up With Ehlers-Danlos Syndrome
EDS is a rare group of genetic conditions caused by collagen-related gene variants. Symptoms can range from joint instability and fragile skin to digestive problems and chronic fatigue. With 13 recognized types, hypermobile EDS is the most common. While EDS has no cure, early recognition, lifestyle support, and personalized medical care can greatly improve quality of life.
References
- https://www.nhlbi.nih.gov/health/postural-orthostatic-tachycardia-syndrome
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6250522/
- https://en.wikipedia.org/wiki/Ehlers%E2%80%93Danlos_syndrome
- https://www.medrxiv.org/content/10.1101/2025.09.19.25336146v1
- https://pmc.ncbi.nlm.nih.gov/articles/PMC5746545/
- https://www.ehlers-danlos.com/prevalence/
- https://pubmed.ncbi.nlm.nih.gov/16278879/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC11213194/
- https://www.ehlers-danlos.com/norris-lab-update-june-2024/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC7785693/
- https://pubmed.ncbi.nlm.nih.gov/38462847/
- https://onlinelibrary.wiley.com/doi/10.1002/ajmg.a.63857
- https://www.mayoclinic.org/diseases-conditions/ehlers-danlos-syndrome/diagnosis-treatment/drc-20362149
- https://pmc.ncbi.nlm.nih.gov/articles/PMC11278074/
- https://hypermobilityclinic.org/nutrition-and-ehlers-danlos-syndrome/
- https://doi.org/10.1186/s12888-016-0922-6
- https://pmc.ncbi.nlm.nih.gov/articles/PMC7882457/
- https://www.dovepress.com/prevalence-of-adhd-and-autism-spectrum-disorder-in-children-with-hyper-peer-reviewed-fulltext-article-NDT
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8425973/
- https://www.verywellhealth.com/ehlers-danlos-syndrome-overview-4782662
- https://www.nature.com/articles/gim201472
- https://www.medicaljournals.se/acta/download/10.1080/00015550410024616/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC6250522/


