Depression is one of the most common mental health disorders worldwide.
Thankfully, it is now possible to handle major depressive disorder and its related symptoms with medications and therapy.
The medications prescribed for treating depression are called antidepressants.
There are different classes of antidepressants available, depending on the drug composition and what they do to the body.
While some people get better from the first day of using antidepressants, others are not so lucky.
They may have to keep trying combinations of medicines before identifying ones that work well.
It may take several months, even years, at times, to narrow down on drugs that work for the person.
Why do antidepressants that work for some have no effect on others?
Genetic makeup could be an important reason why.
According to experts, a person’s genes can influence their response to treatment.
Specific genes may change how a drug is metabolized in the body and, as a result, increase or decrease its effectiveness.
In other words, your genes influence the type and exact dosage of antidepressants you may need to feel better.
Your genes may also influence the risk of side effects from these drugs.
Genetic testing studies your genes and their functions to know how they work and identifies changes/mutations in your DNA, if any.
Pharmacogenomics is the process of testing your genes to understand the body’s response to drugs.
Pharmacogenomics is one of the growing branches of science that is of extreme interest globally.
Some of the popular antidepressants include:
SSRIs are popular as they are better tolerated and have milder side effects. SSRIs also have relatively lesser adverse interactions with other drugs and work by increasing serotonin activity in the brain. Serotonin is a neurotransmitter that is associated with mood regulation and better sleep.
The functioning of this drug is very similar to SSRI, except that this drug acts upon two neurotransmitters - serotonin and noradrenaline. Noradrenaline triggers the fight-flight response in the body.
NASSAs are prescribed if a person doesn’t react well to SSRIs and SNRIs. NASSAs may not cause sexual problems, a common side effect of the above two medications.
TCAs were one of the first antidepressants introduced. These are not very commonly prescribed now because their overdose can turn fatal. In rare cases, people who don’t react to other antidepressants may be prescribed TCAs.
SARIs are also rarely used as primary treatments for depression. They are only prescribed in case other medications don’t work or in case of severe depressive disorder needing a combination of medicines. This drug is effective in treating insomnia and anxiety that are associated with depression.
MAOIs primarily work by preventing the monoamine oxidase enzymes from breaking down neurotransmitters like serotonin and dopamine. By doing this, the levels of these neurotransmitters increase in the brain, leading to a better mood.
MAOIs may lead to severe side effects and are only prescribed if none of the other antidepressants work.
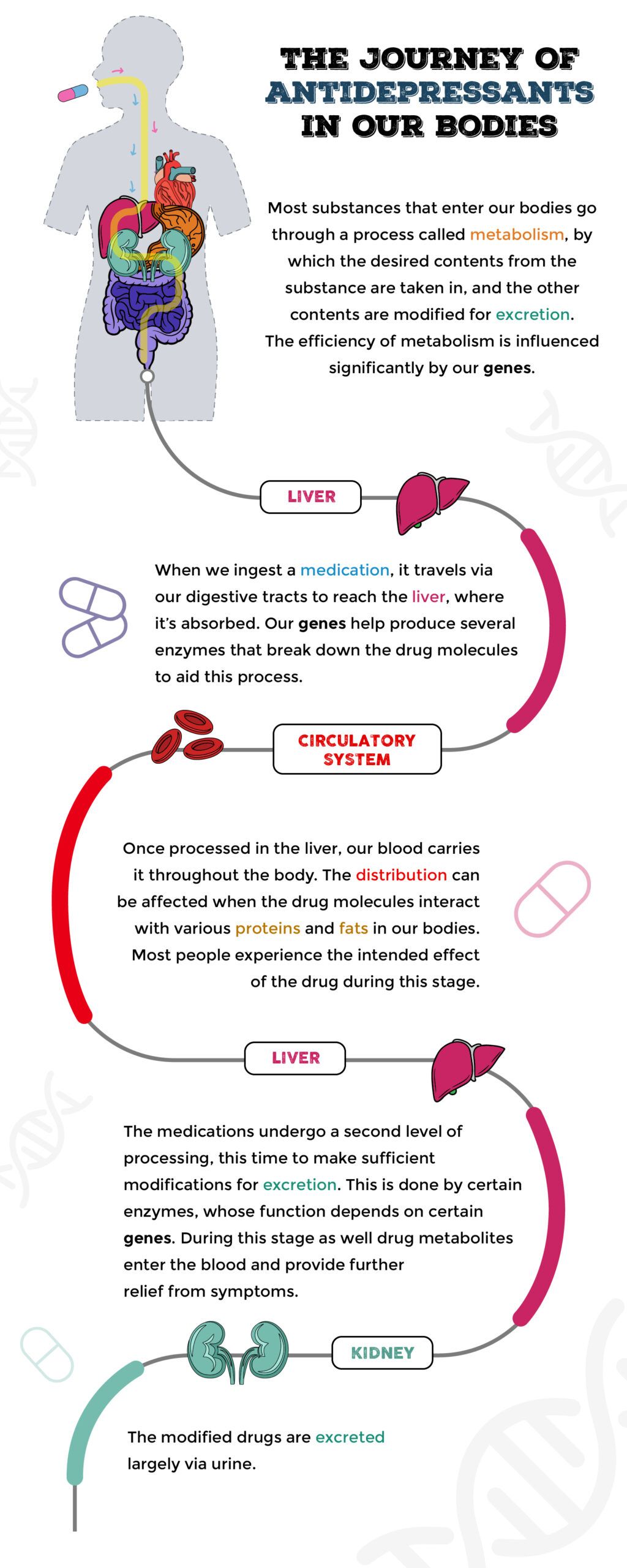
Image: How Do Antidepressants Work
All antidepressants come with side effects. The effect can be mild or severe, depending upon the dosage, the period of use, and the individual’s response to the drug. Some of the side effects common to all these types of antidepressants are:
Without knowing for sure how the person’s body reacts to different antidepressants, the patient may have to waste time trying different combinations of medicines and dealing with their side effects.
Genetic testing may offer insight into what medications could work and reduce the trial-and-error period.
Genetic changes (mutations) cause genes to work differently in every individual, and these changes could do one or more of the following.
Some of the popular genes that could cause these changes are CYP2D6, CYP2C19, SLC6A4, HTR2A, and ABCB1.
While genetic testing can bring about better clarity in using the right drugs, please remember that the field is still growing.
This means that pharmacogenomic testing may not be available for all antidepressants.
Also, apart from genes, other factors could influence your response to a drug, including your age, lifestyle, medications, and health conditions.
According to studies, it may be beneficial to opt for genetic testing when a person has shown low tolerance or has been non-responsive to at least one pharmacological treatment.
Your doctor would be able to help you decide on this.
An individual’s height is many a time associated with health aspects. A good number of studies were carried out to understand if there could be any link between height and alleged health risks. A recent study by a group of researchers from Colorado’s Rocky Mountain medical center confirmed and added more density to those claims. Their study reported that a taller person could have a higher risk of diseases such as peripheral neuropathy or atrial fibrillation.
Height has been associated with health aspects in many past studies.
There is research that talks about how a tall person is happier than a shorter person while a short person lives a longer life than a tall one.
Other analyses have been carried out to understand the risk of diseases if you’re taller than average height.
They included a person’s height as well as other environmental factors affecting it into account.
All such experiments and data are observed to create a more personalized assessment of one’s health.
Researchers suggest that these data can help provide medical advice that is customized to the individual’s genetic makeup and tailor-make treatments. That said, more research needs to be carried out to convert this data into clinical care, says the team.
The phenome-wide study was carried out majorly on the non-Hispanic American population.
The phenome of an individual contains the visible traits - traits that are expressed. In this case, it is the measured height of the participants.
They collected data from the MVP- Million Veteran Program biobank.
The study aimed to understand if a person’s height alone was associated with health risks, not including the environmental factors.
The height of an individual is influenced by two factors – the genes they inherit and the environment they grow in.
They recorded two sets of data, one with genetically-predicted height and the other with contributing environmental factors such as nutrition and economic conditions.
The study tried to find associations to diseases such as coronary heart disease, fat levels, and a few cancers.
Answers to this and more in the Gene Health Report!
The study analyzed over 3000 clinical traits and checked for their correlation to height.
They reported that height does have links to increased or protective disease association.
A tall adult is more susceptible to suffering from peripheral neuropathy or infections of the skin and has lower chances of getting cardiovascular diseases.
In women, they found a strong correlation between asthma and a few peripheral nerve conditions and height.
However, researchers of this study suggested that more such studies were needed to translate this information into medical use.
Your height may be out of your control.
But, changing other aspects of your health isn’t.
The health risks associated with height can be influenced by lifestyle habits which you can change in your favor.
Although tall people are at higher risk for certain diseases, knowing this information can help you detect and avoid them early.
You can make better food choices, sleep differently, and reduce alcohol intake or smoking.
Advanced diagnosis of any disease can surely help to prevent them easily.
While anyone can develop depression, some people are more likely to develop this condition due to the risk factors.
There is no single cause of depression, but several factors contribute to its development.
Common risk factors include:
Depression is found to be more common among women than men.

However, as illustrated above, it doesn’t mean that only women are affected by depression.
Though less common, the consequences of depression are much more severe in men.
Having a first-degree relative with depression may increase your risk of developing the condition.
Twin, adoption, and family studies state that depression has a strong genetic component.
However, how depression genes are passed to the next generation is still unclear.
Sudden changes in life, such as the death or loss of a loved one, the birth of a child, job loss, retirement, etc., may trigger depression in some people.
Some medications have been linked to depression, such as:
Changes in your physical health may impact your mental health.
People struggling with other long-term illnesses like HIV, cancer, chronic liver disease, etc., may develop depression.
People with existing mental health conditions like anxiety are also at a higher risk of depression.
Experiencing mental, physical, emotional, or sexual abuse or trauma may trigger depression.
Around 30% of people who abuse alcohol or drugs have depression.
Depression is in your genes and runs in families.
Children of parents with depression have a high risk of developing the condition.
Though genetics plays an important role, their role is only partial.
40% of depression risk is influenced by genetics, while the rest is due to environmental factors.
Depression occurs due to a complex interplay between genes and the environment, but researchers have not been able to find a single ‘depression gene.’
Genomewide association studies (GWAS) are currently underway to study depression.
Epigenetics, or the study of how and why some genetic codes are expressed as physical or emotional traits, is critical in understanding conditions like depression.
There is no doubt that depression and depressive traits run in families.
A study published in December 2016 found that a child is 70% more likely to develop emotional or behavioral problems if the father shows signs of depression.
This risk is higher if the mother is depressed.
11% of kids are depressed if the father is depressed, and 19% if the mother has the condition.
Around 25% of kids are likely to be depressed if both parents are depressed.
A massive genome-wide association (GWAS) of genetic and health records has identified 178 gene variants associated with major depressive disorder, a condition that affects one in five people.
Genetic variations affect the nerve connections in parts of the brain that control behavior, personality, and decision-making.
The higher the number of variations, the greater the risk of depression.
Inflammatory conditions in the brain cause release of anti-inflammatory chemicals called cytokines.
These cytokines act on the brain to contribute to depression.
When the genes regulating cytokines are involved, they may cause an onset of depression.
You can opt for genetic testing if you feel you are at a high risk of developing depression due to your family history.
Genetic testing may help:
If you have a first-degree relative with depression or showing depressive symptoms, it may be a good idea to seek consultation with your mental health provider.
Undergoing genetic counseling will help you understand your risk for depression and the best way to prevent it.
Understanding that people without genetic or familial history may also develop depression is essential.
At the same time, it is not necessary that people with a risk of developing depression will develop it.
Depression is a serious mental condition that impacts how you feel and the way you think and act.
When left untreated, it can become very disabling, impairing all aspects of human function.
Observational data suggest associations between lower serum vitamin D levels and a higher risk of late-life depression.
Further, lower vitamin D levels may influence the etiology of seasonal affective disorder (SAD).
Some research studies report that people with depression have lower vitamin D levels than those without depression.
But so far, no large-scale study has proven that supplementation with vitamin D or any other vitamin can cure depression.
During exposure to sunlight, the UV-B rays convert a chemical called 7-dehydrocholesterol in the skin into previtamin D3.
Previtamin D3 then travels to the liver and picks up oxygen and hydrogen molecules to become 23-hydroxyvitamin D or 25(OH)D, the active form.
Even though it’s active, 25(OH)D cannot function till it reaches the kidney to acquire the final pair of oxygen and hydrogen.
This forms 1,25 dihydroxyvitamin D/1,23(OH)2D or calcitriol.
Calcium is an integral part of our skeletal system and crucial for bone health.
Vitamin D helps the body absorb calcium.
Without this vitamin, only 10-15% of dietary calcium is absorbed (compared to 30-40% with sufficient vitamin D levels).
Low vitamin D levels can increase the risk of fractures, osteoporosis, and other bone conditions.
Recent studies have observed vitamin D receptors (proteins that bind to vitamin D) in several tissues in the body.
The vitamin D receptors are almost omnipresent from the prostate and heart to blood vessels, muscles, and glands.
Research is still underway to find all the roles of vitamin D in the body.
| Race | Non-Hispanic African-Americans are at the greatest risk for vitamin D deficiency. According to a study, they composed a significant 39.3% of the vitamin D deficient population, compared to only 16.5% of the vitamin D sufficient population. |
| Geography | A study suggests that populations living in any geographic location higher than 35° N are at risk for vitamin D deficiency. Places like North Canada and Alaska, for example, have less access to the UV-B rays. |
| Age | The ability to convert inactive to active vitamin D decreases with age, putting older people at a higher risk for vitamin D deficiency. |
| Skin | Those with darker skin color have more melanin pigments blocking the entry of UV-B rays. Thus, they may be prone to vitamin D deficiency. |
| Pollution | Dust particles can block UV-B rays from reaching the skin. Therefore, those who live in highly polluted may be vitamin D deficient. The deficiency may also be because of the lower inclination to step out in the sun due to higher pollution. |
| Pregnancy & breastfeeding | The demand for vitamin D increases during pregnancy. Following the same diet can result in vitamin D deficiency. Thus, doctors tend to prescribe prenatal supplements with vitamin D in them. |
| Obesity | Fat may interfere with vitamin D absorption. Furthermore, obese people may have mobility issues due to low sun exposure. Those who opt for bariatric surgeries may be at increased risk for malabsorption and subsequent vitamin D deficiency. Those who are overweight but not obese tend to have a lower risk. |
| Absorption issues | Many health conditions like Crohn’s and Celiac disease interfere with nutrient absorption, increasing one’s risk for vitamin D deficiency. |
| Kidney and liver health | The liver and kidneys are two sites in the body where vitamin D is converted into an active and usable form. Any health conditions affecting these organs can increase vitamin D deficiency risk. |
| Smoking | Recent studies have suggested that smoking can reduce vitamin D levels by affecting the ability of sinus mucosa (fluid lining the nasal cavity) to circulate this vitamin. The risk was reduced in former smokers compared to current smokers. |
| Diet | Those who adopt vegetarian and vegan diets without adequate supplementation are at increased risk for vitamin D deficiency. |
| Lifestyle | Any activity that gives less to no room for sunlight can significantly increase vitamin D deficiency risk. Those who wear clothes that cover their whole body for protection or religious reasons get minimal UV-B entry and are prone to deficiency. |
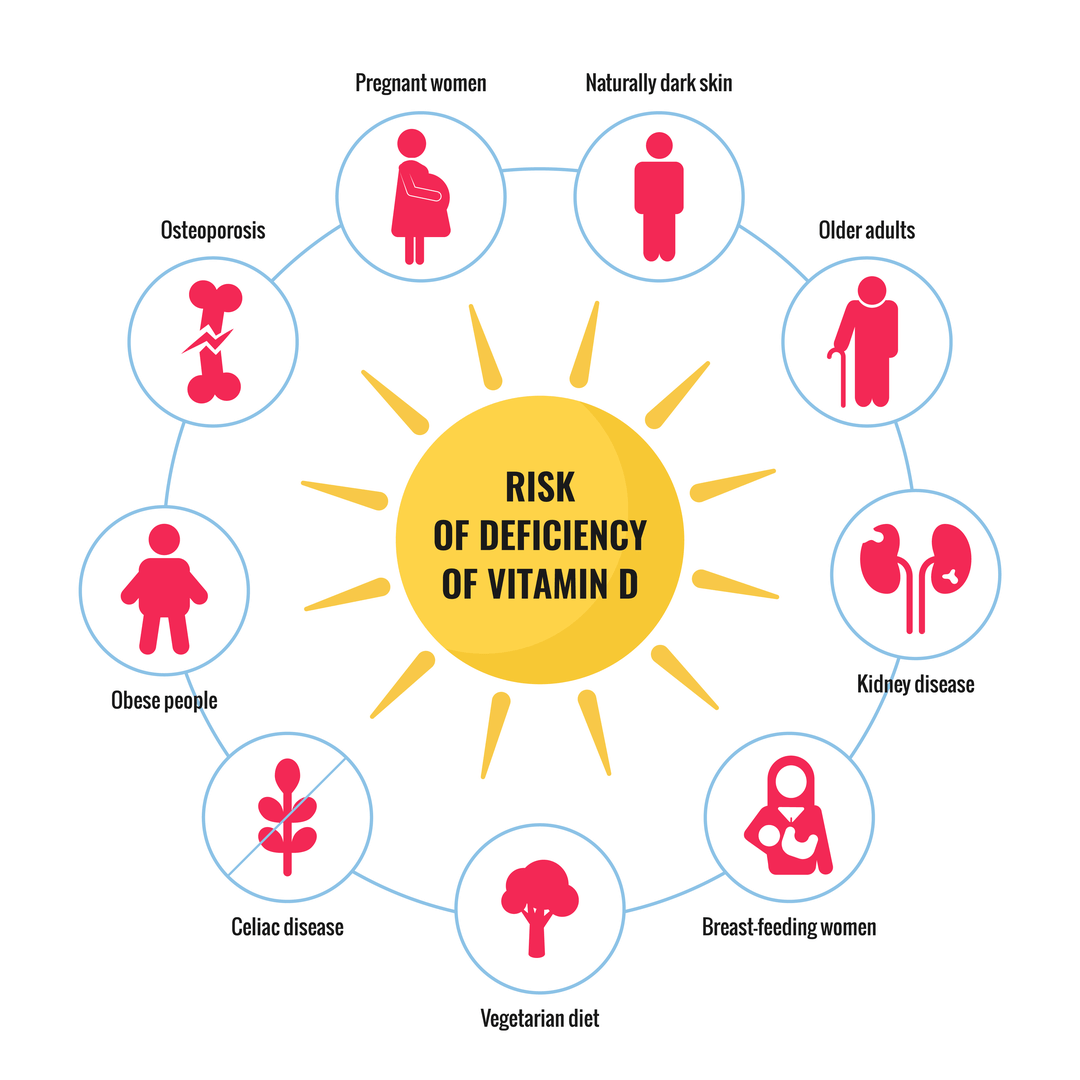
Image: Risk factors for Vitamin D Deficiency
How Much Vitamin D Should I Take? The VDR Gene & Vitamin D Requirements
Numerous studies have reported an association between vitamin D deficiency and depression.
In particular, prenatal vitamin D deficiency has been connected with postpartum depression.
However, whether it is a causation or correlation relationship remains unclear.
A few small studies seemed to have observed improvements in depression symptoms upon vitamin D supplementation.
A review of 14 studies involving 31,424 adults by the National Institutes of Health (NIH) reported low vitamin D levels among those with depression.
However, the clinical trials couldn’t back up such findings.
In August 2020, a large study that observed the link between long-term vitamin D supplementation and depression was published in the Journal of the American Medical Association (JAMA).
The trial included 18,353 participants 50 years and older.
None of them had depression or its symptoms at the beginning of the study.
The trial concluded no statistical difference in “the incidence and recurrence of depression or clinically relevant depressive symptoms” throughout the study in the participants who took vitamin D compared to those who took a placebo.
All these results suggest that the link between vitamin D and depression is a correlative relationship.
Those with depression may have low vitamin D levels, but it doesn’t mean the deficiency causes depression.
Lesser outdoor time
Severe forms of depression can make it very difficult to get out of bed.
Others may go to work but not participate in any outdoor activities.
Such social withdrawal results in lesser outdoor time and consequently lesser exposure to sunlight.
This can result in vitamin D deficiency.
Poor Diet
Some people with depression may lose appetite, putting them at risk of not eating a balanced diet.
They may also not show much interest in looking for vitamin D-fortified foods.
This may increase the risk for vitamin D and other nutritional deficiencies.
Even though the jury is still out regarding vitamin D’s effect on depression, research has shown that it is involved in mood regulation.
This could’ve been derived from the observation that our brains have a widespread distribution of vitamin D.
While you can’t tell for sure that vitamin D supplements can treat or help avoid depression, they may help alleviate the symptoms.
It is important to consult a doctor and get a blood test (if required) before getting started on a vitamin D supplement.
Both vitamin D2 and D3 work well as supplements.
D2 is derived from plants, while animal sources produce D3.
It is important to understand that amping up your vitamin D is not a replacement for seeing a mental health care provider to help treat depression.
We obtain most of the vitamin D via UV-B rays from the sun. Certain food items provide vitamin D as well. Certain groups of the population (dark-skinned, older, living in the northern regions, obese) may be at higher risk for vitamin D deficiency. Though a few small studies have linked vitamin D with depression, there’s still no clarity on whether there’s a causal relationship between the two. Vitamin D may not treat or prevent depression, but studies reveal that supplementation and sun exposure are effective ways to help regulate the mood.
Postpartum depression (PPD) is a condition that affects new mothers (or biological mothers) after childbirth.
About 10–15% of adult mothers yearly are affected by it every year.
Symptoms can include feelings of sadness, emptiness, hopelessness, and worthlessness and can last for weeks or months.
It can make it very difficult for new mothers to care for their babies and lead to sleep, appetite, and mood problems.
The effects on children may include behavioral, developmental, socioemotional, and cognitive delay and may last years beyond infancy.
Studies suggest that individual susceptibility to the development of PPD is related to the presence or absence of certain genetic changes associated with PPD risk.
Till now, hormones have been taught to be the biggest contributor to PPD. Estrogen and progesterone levels increase 10-fold during pregnancy.
The dramatic drop in these hormone levels after childbirth can contribute to the symptoms of PPD.
The levels of thyroid hormones seem to play a role in PPD.
They may also drop after giving birth, contributing to PPD.
Sleep deprivation and early-stage motherhood go hand-in-hand.
This accumulated fatigue can cause a dip in mood and energy.
The symptoms of sleep deprivation and PPD have a lot of overlap that sometimes, it can be difficult to each other apart.
The relationship between sleep and PPD is a two-way street; each can aggravate the other.
According to a study, the risk of depression in women with poor sleep quality was 3.34 times higher than in those with good sleep quality.
Compared to mothers with temporary sleep disturbances, those who consistently report very poor or drastically decreasing sleep quality are more likely to develop PPD.
Other risk factors for PPD are:
Studies show that 1 in 10 dads suffer from PPD.
Research describes certain hormonal changes in dads that promote their attachment to their newborns.
These may include decreased testosterone levels and increased estrogen, prolactin, and cortisol levels.
The hormonal changes may also increase the risk of PPD in men.
Other non-hormonal factors that are involved in PPD include:
Some signs of PPD in men are:
PPD was long thought to be due to the sudden drop in hormones following childbirth.
However, studies have reported nos significant differences in the hormone levels between depressed and non-depressed mothers.
But there’s a possibility that some may be more sensitive to hormonal fluctuations than others.
A group of researchers from Johns Hopkins studied the epigenetic changes introduced in the hippocampus by estrogen.
*epigenetic changes are DNA modifications that turn a gene “on” or “off.”
*hippocampus is a part of the brain governing moods.
They identified the involvement of two genes, TTC9B and HP1B3, in hippocampal activity.
They may regulate the brain’s ability to recognize and adapt to new situations - the two key elements of mood.
Estrogen seems to behave as an antidepressant, supporting the activity of these genes.
The researchers later replicated this experiment in 52 pregnant women with mood disorders.
They note that those with PPD had significant epigenetic changes in those genes that interact the most with estrogen.
This may make them more sensitive to the hormone’s effects.
TTC9B and HP1B3 genes, specifically, were highly correlated with PPD and predicted with 85% certainty about which women got PPD.
Depression is one of the most common mental disorders all over the world. According to experts, one in five people worldwide will experience a major depressive disorder at least once in their lifetime.
In 2020, 14.8 million U.S adults had at least one major depressive disorder that led to the inability to carry out everyday activities.
The brain uses various chemicals to send and receive information.
These chemical messengers are called neurotransmitters.
When there is an imbalance in brain chemical levels, it could lead to multiple mental health problems, including depression.
According to experts, imbalances in three primary monoamine neurotransmitters, dopamine, serotonin, and norepinephrine, can lead to depressive disorders.
Monoamine neurotransmitters are those chemicals with a single amino group.
These are mostly involved in processing emotions, memories, and arousals.
Here are the specific roles of these three neurotransmitters.
A study reported that depression is a combination of two events - loss of a favorable condition and the presence of an adverse situation.
Imbalances in these neurotransmitters can cause a combination of both these events, eventually leading to depression.
Several reasons can cause imbalances in neurotransmitters. Some common ones include:
Genetically, some people may have increased levels of Monoamine Oxidase A (MOA) in the body.
MOA is an enzyme controlled by the MAOA gene.
Higher levels of MOA break down the neurotransmitters and lead to deficient levels of dopamine, serotonin, and norepinephrine in the body.
There are many nutrients needed for producing and regulating neurotransmitters in the body.
Some of them include:
Nutritional deficiencies can hence reduce the levels of neurotransmitters in the body, leading to imbalances.
Lifestyle choices could be another common reason people have serotonin, dopamine, and norepinephrine imbalances.
For instance, chronic sleep deprivation may cause lower serotonin levels, leading to mental health conditions like depression.
Obesity and excessive consumption of sugar are both associated with dopamine deficiency.
Lack of physical activity is also associated with neurotransmitter imbalances.
Some studies suggest that drug abuse during early developmental periods or psychological stress can act as environmental factors, affecting neurotransmitter levels in the body.
Air pollutants may affect neurotransmitter levels in the body, especially serotonin and dopamine.
A study that analyzed suicidal trends in adolescents concluded that suicidal rates were highest when the pollen counts were high.
Image: Causes of Neurotransmitter Imbalance
Get your vitamin and mineral levels checked, and talk to your doctor about supplementing on nutrients that your body may need. Build your diet plan to include all the micro and macronutrients and choose fresher, healthier ingredients to cook with.
A 2015 study suggests that mind-body therapies like yoga and meditation may help handle neurotransmitter imbalances and, as a result, help combat issues like anxiety and depression.
Stress could cause neurotransmitter imbalances in the brain; mind-body therapies can reduce stress and relax the nervous system.
Studies claim that lack of sleep alters neurotransmitter functions in the brain and leads to changes in the production of chemicals like serotonin and dopamine.
Make sure you sleep at least 7-8 hours a day in a comfortable, dark space that allows the secretion of these chemicals.
If you have problems sleeping well, consult your doctor and get help.
Exercising helps release neurotransmitters like dopamine and endorphin.
Exercise also seems to help get better oxygen supply to the brain, allowing the neurons to transmit and receive signals better.
Exercise is a stress reliever, which may help handle norepinephrine imbalances.
Genetic testing may tell you if you are genetically prone to developing neurotransmitter imbalances, thereby having a higher risk for mental health conditions like depression.
Your doctor may be able to help with preventive therapies and solutions to handle the situation, if so.
If you think you show signs of depression, then the first thing to do is get professional help.