People have varying eye colors and shades– from dark to light brown, green, hazel, black, gray, and blue.
In fact, a few people have different colors in both their eyes.
Despite these varying eye colors, you will be surprised to know that there are just two pigments in our eyes - brown and red.
The colored part of the eye is called the iris. The iris contains pigment-forming cells called melanocytes, the same ones present in our skin.
These melanocytes produce two pigments – eumelanin (which is brown-black) and pheomelanin (which is red).
The varying shades of eye color depend upon the amount of pigment produced.
For example, people with dark eye color have a large amount of brown-black eumelanin, whereas those with light blue eyes have very little pigment.
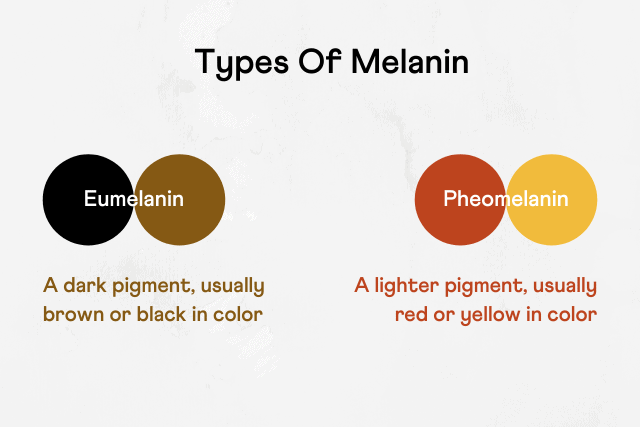
Image: Is Eye Color Genetic: Types of Melanin Pigment
Just like fingerprints, eye color is unique to an individual and is genetically determined.
A genome-wide association study identified 115 genetic variants associated with eye color.
Two genes located close to each other on chromosome 15– OCA2 and HERC2 are said to play an important role in eye color determination.
Though the OAC2 gene influences 75% of eye color, other genes also play a role in melanin production.
The OAC2 gene gives instructions to produce P protein that helps in the maturation of melanosomes (cellular structures that make and store melanin).
The P protein influences the amount of melanin in the iris.
Common changes (called variations or polymorphisms) in the OAC2 gene may reduce the amount of P protein produced.
People with less P protein have less melanin in their eyes.
This also means they may have blue eyes instead of brown.
The HERC2 gene is located very close to the OAC2 gene.
A part of the HERC2 gene is also called intron 86. This region regulates the activity of the OAC2 gene.
At least one polymorphism in the HERC2 gene area has been shown to reduce the OAC2 gene and decrease P protein production.
This results in less melanin in the iris and light-colored eyes.
Though eye color is genetically-determined, it is also an inherited trait.
For a long, scientists believed that a single gene was responsible for an individual’s eye color. However, the inheritance of eye color is far more complex.
The study of inheritance and genetics of eye color are still in the nascent stages.
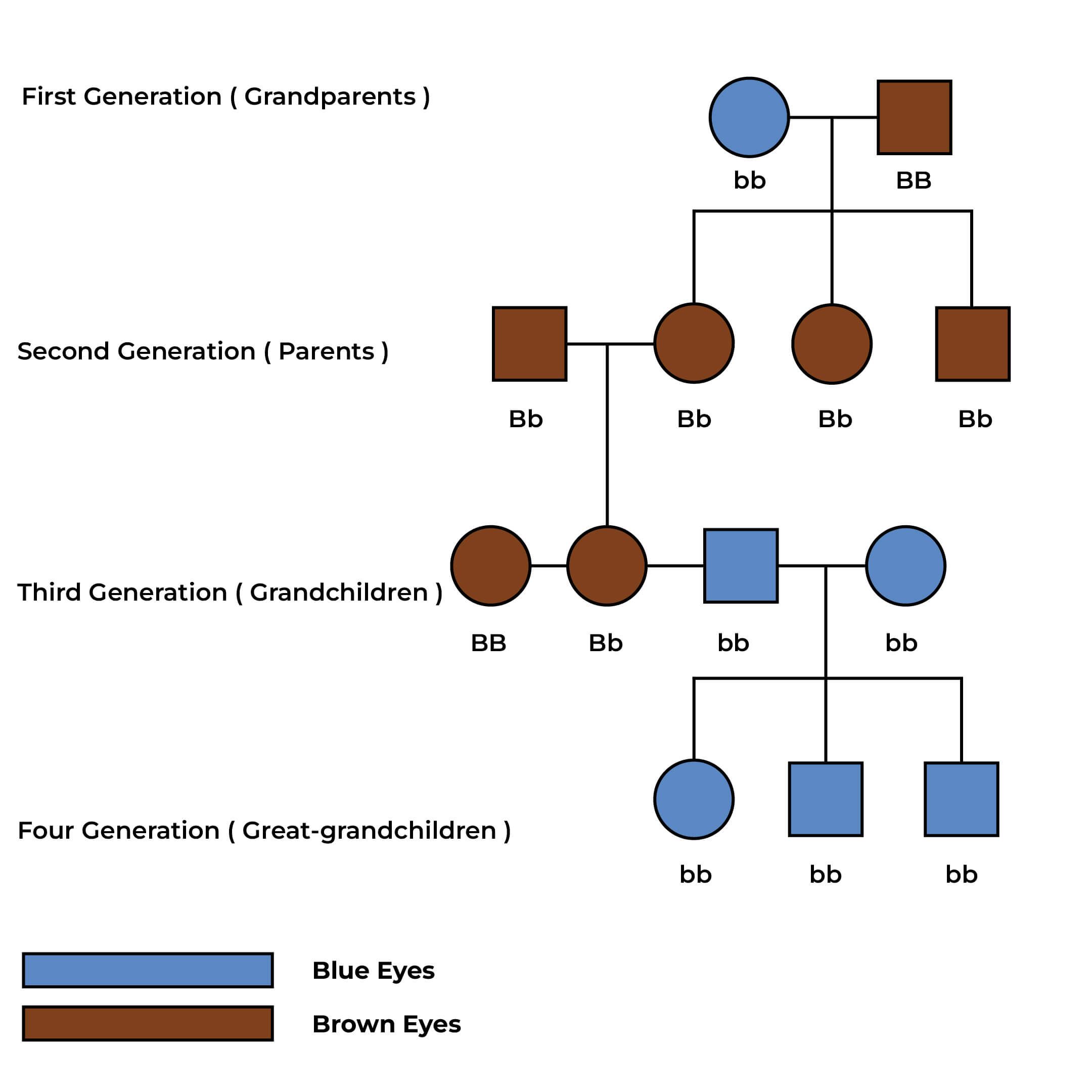
Image: Is Eye Color Genetic: Inheritance of Eye Color
Source: https://www.nature.com/articles/s41433-021-01749-x
It is impossible to predict a baby's eye color with 100% certainty.
But with certain genetic rules, it is possible to make a fair guess.
For example, the brown eye is a dominant trait - this means it can hide traits of green and blue eyes.
To find the possibility of recessive traits, it's helpful to know the grandparents' eye colors.
For example, if the mother has blue eyes and her entire family has blue eyes and the father has brown eyes with his mother and father with brown and blue eyes, the kid will have a 50/50 chance of having a blue-eyed or brown-eyed child.
| Probability of Eye Color | ||||
| Parent 1 | Parent 2 | Blue | Green | Brown |
| Blue | Blue | 99% | 1% | 0% |
| Blue | Green | 50% | 50% | 0% |
| Blue | Brown | 50% | 0% | 50% |
| Green | Green | 25% | 75% | 0% |
| Green | Brown | 12% | 38% | 50% |
| Brown | Brown | 19% | 7% | 75% |
Source: https://www.verywellhealth.com/genetics-of-eye-color-3421603
https://medlineplus.gov/genetics/understanding/traits/eyecolor/
https://www.verywellhealth.com/genetics-of-eye-color-3421603
https://www.gbhealthwatch.com/Trait-Eye-Color.php
A 2020 study identified 5 regions of the genome linked to nicotine dependence.
In the sample report below, we've attempted to analyze some important genes that increase the risk for nicotine dependence.
You can identify your genetic risk of insomnia by using your 23andMe DNA data and placing an order for the Gene Nutrition Report.

Nicotine is a nitrogen-containing chemical and is a highly addictive substance. It is mainly found in tobacco and is primarily consumed by inhaling the smoke of tobacco cigarettes.
Nicotine produces ‘pleasurable and pleasing’ effects on the brain.
With regular smoking, you tend to get used to these positive feelings. Going without a smoke can make you experience unwanted effects - this indicates nicotine dependence.
According to the CDC, smoking is the leading cause of preventable death in the U.S.
A study suggested that smoking is responsible for 1 in every 5 deaths in the U.S.
The symptoms vary amongst individuals and also differ based on the level of dependence. Some signs to watch out for include:
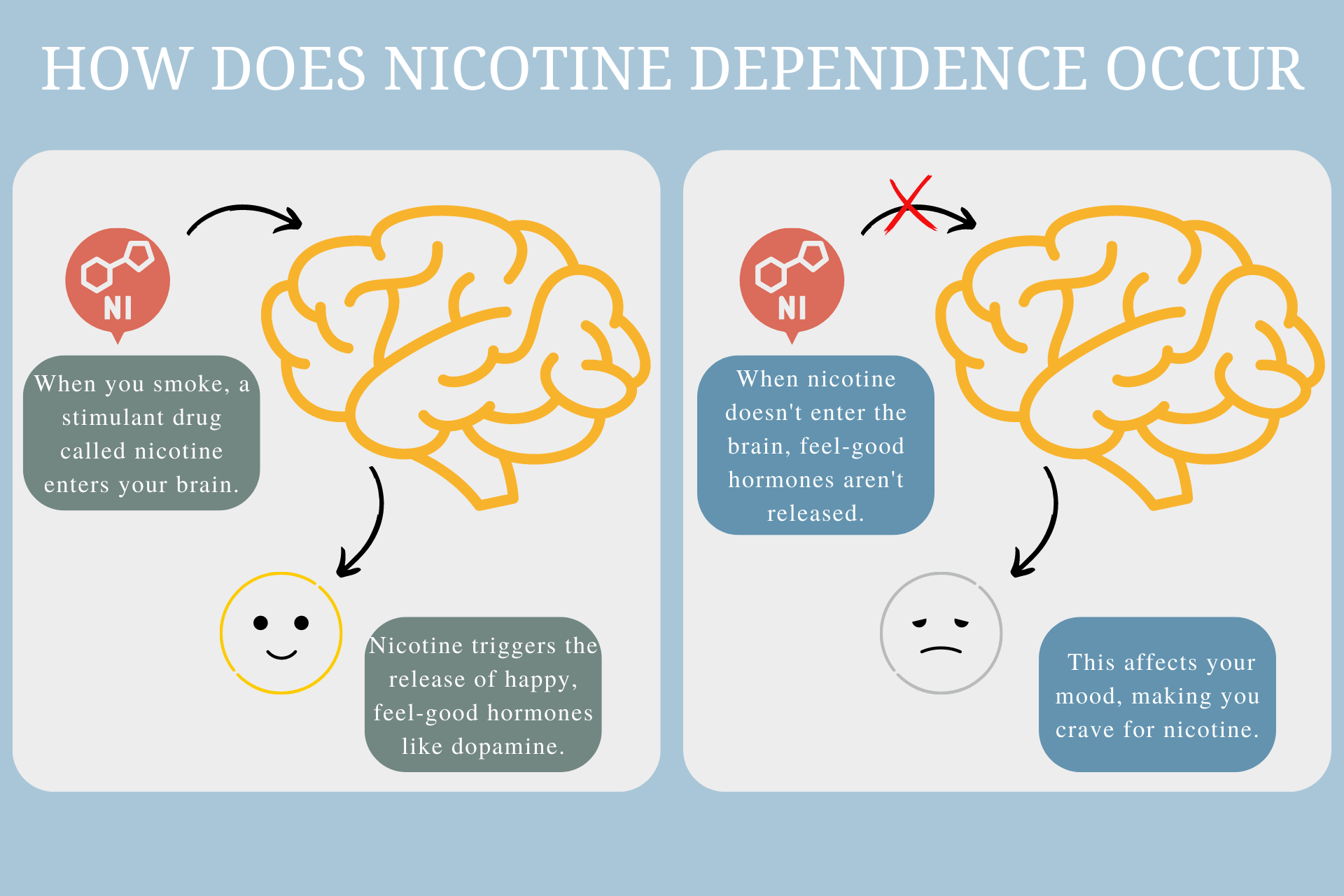
The addictive quality of nicotine is what causes nicotine dependence.
Nicotine triggers the release of the happy hormone dopamine.
This pleasure response is what smokers chase after.
Smoking also increases the heart rate, boosting the noradrenaline hormone. The increased hormone levels enhance mood and concentration.
People who smoke nicotine start craving the dopamine rush. When they abstain from smoking for a few hours, their hormone levels start to drop, and they start to experience undesired effects like irritability and anxiety.
Nicotiana tabacum is the type of nicotine found in tobacco plants. The tobacco plant has been used for its medicinal benefits for at least 200 years.
“It is thought that Christopher Columbus discovered tobacco while exploring America for the first time.
Using tobacco for smoking started and spread rapidly over the 1600s. When it was introduced in Europe, some saw its medicinal purpose, while others viewed it as a toxic, addictive substance.
Tobacco usage exploded when cigarette-making machines were introduced in the 1880s.
Only in 1964 a study established a link between smoking and heart and lung cancer was published. 30 years later, in 1994, the U.S. FDA recognized nicotine as a drug with addictive properties.
Finally, only in 2009 the Supreme Court granted the FDA control to establish some nicotine regulations.
A person may have smoked cigarettes in his youth and would’ve had no trouble stopping it after.
Another person may enjoy recreational smoking but not feel the need to smoke a few every day, and a few others may smoke a pack a day and cannot seem to quit this habit.
So, what contributes to these differences in smoking patterns? Why are the pleasure-inducing effects of nicotine evident in some and not in others?
Some studies have revealed that the differences in response to nicotine can be attributed to changes in some genes that produce receptors to which nicotine binds.
Let’s dilute this further. Nicotine has a similar structure to the neurotransmitter acetylcholine.
Acetylcholine is known to influence memory, arousal, attention, and mood.
Nicotine binds to a type of acetylcholine receptor called the nicotine acetylcholine receptors or nAch. nAch receptor has 5 subunits.
These subunits are produced by certain genes.
Any changes in these genes can alter the structure of the subunits, which in turn can alter the nAch structure.
These alterations modify how you respond to nicotine.
The CHRNA5 gene contains instructions for producing the α5 subunit of the nAch receptor.
Certain changes or mutations in this gene alter the α5 subunit and makes the nAch receptor channels more/less sensitive to nicotine.
rs16969968
rs16969968 is an SNP in the CHRNA5 gene. It influences the pleasurable effects of nicotine.
The A allele has been associated with “enhanced pleasurable responses” to a person’s first cigarette.
The A allele carriers are at an increased risk for nicotine addiction compared to the G allele carriers.
Interestingly, the A allele has also been associated with a lower risk for cocaine dependence!
The CHRNB3 gene contains instructions for producing the β3 subunit of the nAch receptor.
This gene has been identified to predispose an individual to nicotine addiction.
rs10958726
rs10958726 is an SNP in the CHRNB3 gene. The T allele of this SNP has been associated with an increased risk of nicotine dependence.
Several other genes like CHRNG, CHRNA4, CYP2B6, and FMO also influence the risk of nicotine dependence.
Age: According to a study, the chances of developing nicotine dependence are higher when the age of onset of smoking is before 21, especially between 18-20 years.
Peers: People who grow up with smoking parents or spend more time around friends who smoke are more likely to smoke and may eventually develop nicotine addiction.
Substance usage: People who consume alcohol or drugs are more likely to become nicotine dependent. The reverse relationship is also true! In fact, according to a study conducted to evaluate concurrent use of alcohol and cigarettes, approximately one-third of current drinkers smoked, whereas approximately 95 percent of current smokers used alcohol.
Mental illness: People with mental troubles like depression, PTSD, or schizophrenia are more likely to be smokers than others. A study examining depression and nicotine dependence from adolescence to young adulthood reported that depression is a prominent risk factor for nicotine dependence. The adolescent and youth population exhibiting depression symptoms constitute an important group that requires smoking intervention.
Using tobacco can lead to grave health complications. Nicotine dependence has been tied to an increased risk of various health conditions.
Tobacco smoking, to date, remains the most established contributor to lung carcinogenesis or lung cancer.
Recent studies suggest that nicotine, in small quantities, accelerates cell growth and, in large quantities, becomes toxic to cells.
Nicotine also decreases the levels of CHK2, a protein that acts as a tumor suppressor.
Further, it lowers the effects of anti-cancer treatments. Smoking contributes to 30% of all deaths due to cancer!
Cigarette smoking remains the leading cause of COPD in the U.S.
A CDC analysis revealed that the prevalence of COPD in adults was 15.2% among current cigarette smokers, compared to 2.8% among adults who never smoked!
Smoking causes damage to the heart and blood vessels.
It also alters your blood chemistry, contributing to plaque build-up. In the U.S., smoking accounted for 33% of all deaths caused due to cardiovascular diseases.
Research shows that nicotine influences the activity of the pancreas.
The usage of nicotine leads to decreased production of insulin by the pancreas.
Thus, the blood sugar levels are poorly regulated, leading to diabetes.
Smokers with diabetes may require higher insulin doses to keep their blood sugar levels in check.
Tobacco smoking during pregnancy increases the risk of morbidity and mortality in newborns.
Nicotine damages the developing lungs and brain of the fetus.
Common birth defects caused due to nicotine are cleft lip and cleft palate.
Nicotine Replacement Therapy (NRT) has been suggested for pregnant women who cannot quit smoking.
However, the safety of NRT to the developing fetus has not been well-documented yet.
Nicotine withdrawal is the set of symptoms one experiences upon stopping tobacco usage. It can start as early as 30 minutes from the last usage.
The range and severity of symptoms can depend on how long the person has been smoking and how often they have smoked.
Owing to the withdrawal symptoms, quitting smoking can be very challenging.
The following are the basics of any de-addiction program which can help you overcome nicotine addiction.
Other specific ways can help you gradually become nicotine-independent.
It is the process of administering the nicotine that your brain demands more safely by avoiding all the other harmful substances present in cigarettes.
This also provides relief from the withdrawal symptoms.
NRT supplies lower doses of nicotine at slower rates. Some of the commonly available NRTs include:
All of these are generally available over the counter and do not require prescriptions.
Certain medications do not contain nicotine but are designed to produce the same effects of nicotine on the brain.
They help decrease cravings and alleviate other withdrawal symptoms. Some examples of these medications include Chantix and Zyban.
Important note
In 2009, the FDA mandated the makers of such medications to put a black box, warning the users about the possible dangerous psychological effects, including agitation, depression, and suicidal thoughts.
CBT trains smokers to cope with the symptoms of withdrawal. CBT has achieved twice the success rate when quitting smoking (compared to people who didn’t receive CBT).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2928221/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2928221/
https://www.ncbi.nlm.nih.gov/pubmed/18783506?dopt=Abstract
https://www.snpedia.com/index.php/Rs16969968
https://www.ncbi.nlm.nih.gov/pubmed/18519132?dopt=Abstract
https://www.ncbi.nlm.nih.gov/snp/rs10958726
https://www.cdc.gov/pcd/issues/2020/19_0176.htm
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1931414/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4314348/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4553893/
https://www.cdc.gov/mmwr/volumes/68/wr/mm6824a1.htm
https://www.ncbi.nlm.nih.gov/books/NBK53012/
https://www.sciencedaily.com/releases/2019/10/191016131214.htm
https://medlineplus.gov/ency/article/007438.htm
Answering whether PTSD (post-traumatic stress disorder) is genetic can be challenging.
While studies suggest that genes may play a role in 30% of cases, the complex interplay between genes and the environment makes it difficult to pin down specific gene variants.
In addition, PTSD often occurs alongside other mental illnesses, making it even harder to tease apart the relative contributions of genetics and environment.
One way scientists have tried to untangle the role of genes in PTSD is through genome-wide association studies (GWAS).
These studies look for small variations in the DNA of people with and without PTSD to identify gene variants that might be linked to the disorder.
PTSD is a mental and behavioral disorder that can occur after someone experiences or witnesses a traumatic event.
Some of the common PTSD are flashbacks, nightmares, trouble sleeping, and feeling angry or irritable.
For some people, the symptoms get worse and last for a long time, even years.
PTSD affects how a person thinks and feels and may present as a change in their personality.
When a person experiences or witnesses a traumatic event, it can have a lasting effect on their mental health.
PTSD symptoms can appear soon after the traumatic event or may not appear until months or even years later.
PTSD can cause a person to feel scared, anxious, and isolated. It can also lead to physical health problems.
If you are experiencing symptoms of PTSD, it is important to seek help from a mental health professional.
A terrifying event can trigger PTSD.
PTSD can occur after any dangerous or scary encounter, such as a car accident, natural disaster, terrorist attack, or sexual abuse.
It can also occur after witnessing someone else experience a traumatic event or learning that a loved one has been harmed.
A report from Harvard University shows that 30 percent of PTSD cases were explained by genetics.
According to the study, identical twins with smaller hippocampus were more likely to develop PTSD following tragic events.
The study further reported that symptoms of PTSD overlap with those of other psychiatric conditions like panic disorder and generalized anxiety disorder.
Genes that play a role in creating "fear memories" could be targets for potential therapeutic interventions for PTSD.
In 2019, scientists from the University of California San Diego School of Medicine and more than 130 additional institutions participating in the Psychiatric Genomics Consortium conducted the largest and most diverse genetic study of PTSD to date.
They used a genome-wide association study (GWAS) to study genetic data points across 200,000 people.
According to the authors, 5-20% of the variability in PTSD risk following a traumatic event.
The study team also reports that, like other psychiatric disorders, PTSD is highly polygenic - it is associated with thousands of genetic variants, each making a small contribution to the disorder.
Karastan Koenen, the senior author, also said, "based on these findings, we can say with certainty that there is just as much of a genetic component to PTSD risk as major depression and other mental illnesses."
After evaluating certain symptoms, a qualified healthcare professional can help with PTSD diagnosis.
To be diagnosed with PTSD, the following criteria should be met:
These symptoms also must:
Psychotherapy and medications are commonly used treatment options for PTSD.
Researchers have identified a number of genes associated with Alzheimer's disease.
While some genes increase your risk for developing Alzheimer's (risk genes), others are causal (deterministic).
In the sample report below, we've attempted to analyze some important genes that increase the risk for Alzheimer's.
You can identify your genetic risk of Alzheimer's by using your 23andMe DNA data and placing an order for the Gene Health Report.

According to the Alzheimer’s Association, Alzheimer’s disease is “a type of dementia that causes problems with memory, thinking and behavior.”
The disease is named after Dr. Alois Alzheimer, who first described it in 1906.
Symptoms usually develop slowly and worsen over time, eventually interfering with daily tasks.
It is caused due to a combination of different factors.
The risk for Alzheimer's disease has a genetic component to it.
While there is no current cure for Alzheimer’s, treatments are available to help manage the symptoms.
There are two types of Alzheimer’s Disease: early-onset and late-onset.
Early-onset Alzheimer’s is a rare form of the disease that typically affects people in their 40s and 50s.
Late-onset Alzheimer’s is the more common form of the disease and typically affects people over the age of 65.
Both forms of Alzheimer’s are progressive, meaning they worsen over time.
Early-onset Alzheimer’s progresses more rapidly than late-onset Alzheimer’s, but both forms ultimately lead to dementia.

The cause of Alzheimer's is still largely unknown, but scientists believe it is linked to a combination of genetic, lifestyle, and environmental factors.
One of the main theories behind the development of Alzheimer's disease is the build-up of abnormal proteins (amyloid plaques and tau proteins) in the brain.
This build-up damages the nerve cells and prevents them from communicating with each other.
When the brain cells get affected, the levels of neurotransmitters or brain chemicals used to send messages in the brain decrease.
One of these brain chemicals, called acetylcholine, is involved in learning and memory.
In the brains of people with Alzheimer’s, the levels of acetylcholine are lower.
As there is more and more plaque build-up, the brain cells die, causing the brain to shrink.
Although there is no cure for Alzheimer's, treatments are available to help slow its progression and improve the quality of life for those with it.
Both types of Alzheimer’s have a genetic component to it.
While some genes increase the likelihood of a person developing the condition, others guarantee disease development.
Most people with Alzheimer’s have the late-onset type.
The most commonly identified gene for this type is the ApoE gene, which is involved in making a protein that helps carry cholesterol and other types of fat in the bloodstream.
ApoE comes in different forms determined by the alleles e2, e3, and e4.
About 25 percent of people carry one copy of APOE ɛ4, and 2 to 3 percent carry two copies.
Some other genes that influence late-onset Alzheimer’s risk are (list not exhaustive):
10% of all people with Alzheimer’s have the early onset type.
Research has identified 3 genes associated with this condition.
The APP Gene
The APP gene contains instructions for producing the amyloid precursor protein.
It is present throughout the body, mainly in the brain and spinal cord.
This protein is important for brain development and helps nerve cell movement and communication.
10-15% of early-onset Alzheimer’s is due to mutations in the APP gene.
The PSEN1 Gene
The PSEN1 gene contains instructions for producing presenilin 1, a protein that is a part of a larger complex called the gamma-secretase.
This complex plays a role in the fragmentation of proteins, especially the amyloid precursor protein.
Mutations or changes in the PSEN1 gene can result in abnormal chopping of the APP, resulting in amyloid plaque buildup, an important cause of Alzheimer’s.
The PSEN2 Gene
The PSEN2 gene produces presenilin 2 and works in a similar fashion to the PSEN1 gene to contribute to Alzheimer’s risk.
There is no cure for Alzheimer’s disease; however, there are medications that can help to slow the progression of the disease and manage symptoms.
The U.S. Food and Drug Administration (FDA) has approved several medications for treating Alzheimer’s, including cholinesterase inhibitors and memantine.
These medications can help improve cognition, memory, and communication skills and reduce behavioral problems.
Clinical trials are ongoing to test new potential treatments for Alzheimer’s disease.
Whether it is genetics or environment that plays a role in determining intelligence has always remained an important question.
This is a controversial topic in the history of psychology, and to date, new studies have come up trying to understand the relationship between genetics, environment, and human Intelligence Quotient (IQ).
Many such studies conclude that a significant part of human intelligence is genetically influenced.
However, the same studies suggest that the environment may still play a role in molding the genetic trait.
One of the earliest studies that attempted to understand genetic influences on IQ was the twin studies by professor Sir Cyril Burt.
His studies, published between 1943 and 1966, concluded that genetics might significantly influence IQ levels.
Other recent studies claim that the heritability of intelligence could be as high as 0.8 (on a scale of 0.0 to 1.0).
Some of these studies examined the IQ scores of monozygotic (identical) twins and dizygotic (fraternal) twins.
Monozygotic twins share 100% of their genetic material, while dizygotic twins may share an average of 50% of their genetic material.
These studies reported that the IQ scores of monozygotic twins are more similar than that of dizygotic twins.
In a household with biological and adopted siblings, the IQ levels of biological siblings may be more similar to that of adopted siblings.
This also points to the fact that genetics may play a more prominent role in influencing IQ levels.
There is no single gene that controls intelligence levels. Instead, a person’s intelligence may depend on interactions between multiple genes.
A UK-based study analyzed the DNA variants from more than 240,000 people and reported that up to 538 genes might be associated with intelligence.
That is why intelligence is called a polygenic trait.
Studies ascertain that 30-75% of variations in people’s IQ levels could be genetically driven.
However, environmental influences may help or prevent a person from achieving the genetic potential of IQ levels.
Socioeconomic status refers to the family or individual’s access to economic resources like money and their position in society.
According to experts, poverty or lack of financial stability may prevent a child from reaching their full genetic potential of intelligence.
A research paper analyzed the IQ levels of children from different SESs.
According to the results, children of the highest and lowest SES backgrounds were, on average, separated by 6 IQ points at the age of 2 years.
Further, by the age of 16, the IQ gap had almost tripled.
Lack of nutrition affects IQ levels, especially in the initial few years of a child’s life. According to a study, malnutrition between the ages of 1 and 5 may reduce IQ levels by up to 15 points.
Cognitive stimulation includes a variety of experiences the child has at home. Here are some cognitive influences affecting IQ levels.
A study states that educational duration and IQ levels could be closely related.
According to it, intelligence increases by 1 to 5 IQ points for every additional year of education.
A significant part of a person’s intelligence is inherited by birth.
30-75% of variations in IQ levels could be due to genes, and multiple genes play a role in determining the intelligence potential of the individual.
However, environmental factors may influence how much of the genetic potential the person achieves during the lifetime.
For instance, a child could be born with high intelligence. However, environmental factors like low SES, malnutrition, or lack of right education may affect the child’s IQ.
For a person to have high IQ levels, genetics and the environment must be favorable.
The anxiety or anticipation of fear may make one more sensitive to pain, and this phenomenon is common in people with chronic pain.
Fear sets off a fight or flight mode in the brain.
When we are under fear, the body transfers its healing abilities to fight the possible danger.
In this situation, it is natural for us to become hypervigilant, and we begin perceiving even the slightest sensations more intently.
Each of us responds to pain differently.
Fear and anxiety about pain may influence an individual’s variation in how much they feel pain.
Most people develop a negative feedback loop around pain based on what they hear, see, or experience.
The brain starts storing these stimuli as long-term memory, called fear conditioning.
These stimuli, such as smell, sound, weather, or images, act as triggers, and the individual begins to react to them negatively.
Depending upon the grade or severity of fear, people may experience a rise in blood pressure, tense feelings in the body, etc.
Fear activates a part of the brain called the amygdala.
The amygdala is responsible for processing emotions and triggers the ‘fight’ or ‘flight’ response.
Constant worry and anxiety affect the individual’s cognition and emotions.
In a way, fear takes over the brain’s functioning, and we are mentally or physically hostages of this fear.

Image: Parts of the brain involved in fear response
Inspired from https://science.howstuffworks.com/
Though fear originates and is primarily influenced by the brain, your genes may also have a role to play in it.
Many specific genes, interactions between genes and environment, and biological pathways have been associated with pathological fear and anxiety disorders.
A study conducted to understand the fear of dental pain showed that while dental fear was 30% heritable, the fear of pain was 34% heritable.
A GWAS (genome-wide association study) was carried out in 2017 that included 990 individuals to dig more into the heritability and genetics of fear of pain.
This study aimed to identify the genes that could potentially drive the heritability of fear of pain.
The study reported 3 genome-wide significant genetic regions (loci) regulating fear of minor pain.
Numerous other genetic associations were observed for general fear of pain, fear of severe pain, and fear of medical/dental pain.
The researchers identified the following genes near the genetic loci associated with fear of pain:
The transmembrane protein 65 (TMEM65) gene was particularly interesting as it was associated with musculoskeletal pain in humans (pain due to muscle or bone injury).
This gene is also implicated in abnormal pain threshold and predisposition to neuropathic pain in rats.
Neuropathic pain can happen if your nervous system is damaged or not working correctly.
The NEFM and NEFL genes are also of interest since they regulate neuronal functioning, especially motor neurons.
Motor neurons are a type of brain cell located within the spinal cord and the brain.
They’re involved in transmitting pain signals.
Hence, these two genes may be related to the pain experience.
The study concluded that even though there were several associations observed for general fear of pain and fear of severe pain, the associations observed for fear of minor pain had stronger statistical evidence.
The fear of pain is a combination of genetic and environmental factors.
There is no way to prevent fear of pain.
People with a greater fear of pain must find ways to alleviate this fear to live normal, productive lives.
Yoga, meditation, breathing techniques, visualization, and mindfulness activities are great examples of simple exercises you can do from the comfort of your home.
For people who require professional help for their pain-related fear, cognitive behavioral therapy, exposure therapy, and physical exercises may be helpful.
Exercise and fitness activities release serotonin and other chemicals in the brain that improve your mood and enable you to manage pain effectively.
With the right treatments, most people can manage their fear of pain.