Estimated reading time: 18 minutes
Irritable bowel syndrome (IBS) is a chronic functional gastrointestinal disorder defined by recurring abdominal pain and changes in bowel habits.
Affecting 10 to 15 percent of adults worldwide, it is one of the most commonly diagnosed digestive conditions. [1]
Unlike inflammatory bowel disease (IBD), IBS causes no visible structural damage to the gut.
Instead, it reflects a dysfunction in how the gut and brain communicate.
The gut contains more nerve cells than the spinal cord and produces over 90 percent of the body's serotonin.
When the two-way communication network between the digestive system and the brain, known as the gut-brain axis, becomes dysregulated, ordinary digestive sensations can register as pain.
In Western countries, women are approximately twice as likely as men to have IBS, and among those who seek medical care for it, the female-to-male ratio is roughly 2 to 2.5 to 1. [2]
This gap appears around puberty and is most pronounced during the reproductive years. As women pass menopause, IBS rates gradually decline and begin to converge with those of men. [3]
Writing in Gastroenterology, researchers from the Mayo Clinic noted that slow gastric emptying and colonic transit are more common in healthy women than men, contributing to the female preponderance of constipation-related GI symptoms. [3]
"Women tend to report more bloating, indigestion, and nausea than men. Hormonal changes across a woman's life, and differences in anatomy, play a real role in how gastrointestinal symptoms develop and persist."
— Dr. JoAnn Hong-Curtis, MD, Gastroenterologist, Yale Medicine
While IBS affects everyone differently, consistent and reproducible patterns have emerged from decades of research comparing how men and women experience the condition.
A meta-analysis and a major review published in PMC (National Institutes of Health) found that women with IBS are significantly more likely to report abdominal pain, constipation, bloating, abdominal distension, and nausea.
Women also report more extraintestinal symptoms: fatigue, bladder sensitivity, and musculoskeletal pain that goes beyond the gut. [2]
According to a review published in The American Journal of Gastroenterology (PMC), women with IBS are also more likely to have coexisting anxiety and depression compared with men who have IBS.
These psychological symptoms can amplify gut pain signals through the gut-brain axis. [3]
Men with IBS are significantly more likely to experience diarrhea-predominant IBS (IBS-D).
A large pooled analysis found IBS-D prevalence of 50 percent in men versus 31 percent in women, while IBS-C was far more common in women at 40 percent versus 21 percent in men. [2]
Men with IBS also tend to report lower levels of psychological distress and fewer extraintestinal complaints.
However, some researchers note this may partly reflect differences in how symptoms are disclosed rather than true biological differences.
| Expert picks: What To Read Next |
|---|
| Your Smartwatch Can Now Predict IBS Flare-ups |
| What Are Some Simple Tests You Can Do To See If You’re Aging Well? |
A landmark December 2025 study from UC San Francisco, published in the journal Science, identified the specific cellular mechanism by which estrogen amplifies gut pain in females.
Researchers led by Dr. Holly Ingraham and 2021 Nobel Laureate Dr. David Julius found that estrogen receptors cluster in L-cells in the lower colon, triggering a cascade that releases serotonin and activates pain-sensing nerve fibers.
When male mice were given estrogen to match female levels, their gut pain sensitivity rose to match that of females. [4]
"Instead of just saying young women suffer from IBS, we wanted rigorous science explaining why."
— Holly Ingraham, PhD, Herzstein Professor of Molecular and Cellular Pharmacology, UCSF
"We knew the gut has a sophisticated pain-sensing system, but this study reveals how hormones can dial that sensitivity up by tapping into this system through an interesting and potent cellular connection."
— David Julius, PhD, Nobel Laureate in Physiology or Medicine, UCSF
Earlier foundational work, published in PubMed, confirmed that variations in ovarian hormones across the menstrual cycle affect sensorimotor GI function.
This was observed in both healthy individuals and those with IBS.
These variations appear to modulate pain processing through neuromodulator systems and emotional pain pathways. [5]
Dr. Mindy Lee, MD, Assistant Professor of Clinical Medicine in Gastroenterology and Hepatology at Weill Cornell Medicine, explains that before menstruation, high estrogen and progesterone levels cause increased bloating and constipation.
Once hormone levels fall at the onset of menstruation, women tend to shift toward diarrhea and increased pain sensitivity. [6]
"In general, immediately before a woman menstruates, there's a higher level of estrogen and progesterone that causes more bloating and constipation. Then hormone levels start to fall at the onset of menstruation, and during their periods, women tend to have more symptoms of diarrhea and increased pain sensitivity."
— Dr. Mindy Lee, MD, Weill Cornell Medicine
This cyclical pattern is one of the most well-replicated findings in IBS research and helps explain why many women feel that their gut and their cycle move in lockstep.
Pregnancy brings sustained high levels of progesterone, which inhibits smooth muscle contraction and slows gut motility considerably. Nearly a third of pregnant women experience increased constipation, particularly during the last trimester. [7]
Two studies presented at the American College of Gastroenterology (ACG) 2024 Annual Scientific Meeting found that hormone replacement therapy (HRT) in postmenopausal women is associated with increased risk of developing IBS and gastric motility disorders, elevated GI symptoms, and greater medication use. [8]
"In the GI clinic that I work in, we see an increased population of women that come in with functional GI disorders, and I think there is a huge need for continued research really paying attention to what other things potentially could be contributing to this."
— Dr. Jacqueline Khalil, DO, Case Western Reserve University/MetroHealth, ACG 2024
Dr. Mark Pimentel, Executive Director of Cedars-Sinai's Medically Associated Science and Technology Program, has noted that women in menopause have a different gut microbiome compared to premenopausal women, and that HRT appears to make the microbiome look younger in composition, though the clinical significance for IBS is still being studied. [9]
Women with IBS report higher rates of anxiety, depression, and a history of trauma compared with men who have IBS.
Chronic stress elevates cortisol, and research by Heitkemper and colleagues found that cortisol was unusually elevated in women with IBS. A separate Italian study confirmed exaggerated cortisol activity in IBS patients compared to controls. [10]
This does not mean IBS is a psychological condition. It means the brain and gut are biologically connected, and that psychological state has real, measurable effects on gut physiology.
Getting the right diagnosis matters. Several conditions share symptoms with IBS and are more likely to affect people assigned female at birth.
Researchers and clinicians consistently flag these conditions as common sources of misdiagnosis.
Stress is the most consistently reported trigger for IBS flare-ups in the clinical literature.
Activation of the hypothalamic-pituitary-adrenal (HPA) axis during stress elevates cortisol levels, which dysregulates gut motility and heightens visceral sensitivity.
A landmark study by Dr. Douglas Drossman and colleagues at UNC Chapel Hill, drawing on a national survey of 5,430 US households, found that IBS was more prevalent and more stress-sensitive in women than men during the reproductive years. [10]
Even anticipatory stress, such as worrying about a social event or a medical appointment, can trigger symptoms.
Chronic stress, anxiety, and unresolved trauma can physically rewire how the nervous system processes gut signals.
Triggers vary considerably from person to person, but the most widely reported ones include:
The low-FODMAP diet, developed by researchers at Monash University in Australia, is one of the most evidence-based dietary approaches for IBS.
In clinical trials, it has produced meaningful symptom improvement in 50 to 80 percent of IBS patients.
The National Institute for Health and Care Excellence (NICE) recommends it as a second-line dietary intervention when general dietary advice is insufficient. [11]
| Expert pick: What To Read Next |
|---|
| The Ultimate Guide To Anti-inflammatory Diet + Food List PDF |
As described above, the sharp drop in estrogen and progesterone before menstruation is a consistent and well-documented trigger.
Tracking symptoms alongside the menstrual cycle can help identify patterns and guide both self-management and clinical decisions.
IBS stool appearance varies by subtype.
Clinicians use the Bristol Stool Chart, a validated seven-point visual scale, to categorize stool consistency:
People with IBS-M may move between hard and loose stools, sometimes within the same day.
Stools in IBS do not typically contain blood.
If you notice rectal bleeding, significant amounts of mucus, unexplained weight loss, or symptoms that wake you from sleep, contact a healthcare provider promptly, as these are red flags that require investigation.
Medical Disclaimer
The strategies listed below are for general informational purposes only. They are not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before trying new remedies, supplements, or over-the-counter medications, especially if you are pregnant, breastfeeding, taking other medications, or managing another health condition.If your flare-up is severe, prolonged, or accompanied by fever, rectal bleeding, or significant weight loss, seek medical attention promptly.
When a flare strikes, the following approaches can ease symptoms in the short term:
Dr. Mindy Lee of Weill Cornell Medicine notes that certain medications work better in women than in men, including alosetron (a 5HT3 antagonist approved for women with severe IBS-D) and tegaserod (a 5HT4 agonist). [6]
Other prescription options include:
Prescription Medications: Important Notice
All medications listed in this section are prescription-only and must be prescribed and monitored by a licensed healthcare provider. Do not start, stop, or adjust any prescription medication without first speaking to your doctor. Some medications listed here (such as alosetron) carry specific risk warnings from the FDA and are only prescribed under restricted programs. This information is not intended to replace a consultation with a gastroenterologist or your primary care physician.
Cognitive behavioral therapy (CBT) and gut-directed hypnotherapy both have strong evidence for reducing IBS symptom severity, as recognized by the American College of Gastroenterology. [13]
"The most important thing is a willingness to work with your physician and try different treatments to see what works best for you. That may require a lot of patience. But IBS is something that can be controlled. With the right course of treatment, you can lead a normal life."
— Dr. Dasha Moza, MD, Gastroenterologist, Rochester Regional Health
General Wellness Information: Not Medical Advice
The lifestyle and supplement recommendations below reflect general evidence-based guidance and are not personalized medical advice.Individual responses to dietary changes, probiotics, and exercise vary widely. What works for one person may worsen symptoms for another. Before starting a restrictive diet such as the low-FODMAP diet, consult a registered dietitian experienced in gastrointestinal health. Unsupervised dietary restriction can lead to nutritional deficiencies. Speak with your doctor before adding any new supplement, including probiotics or fiber supplements, particularly if you are on medications or have other health conditions.
Certain probiotic strains, particularly Bifidobacterium and Lactobacillus species, have shown benefit for bloating and overall symptom scores in some trials, though results across studies are inconsistent.
Because the gut microbiome is highly individual, finding the right probiotic may take trial and error under the guidance of a gastroenterologist or dietitian.
Soluble fiber supplements such as psyllium husk can help regulate bowel habits in both IBS-C and IBS-D.
Insoluble fiber, such as wheat bran, can worsen symptoms for some people and should be introduced cautiously.
This question is increasingly common in clinical practice as GLP-1 receptor agonists such as semaglutide (Ozempic, Wegovy) become more widely used for type 2 diabetes and weight management.
GLP-1 medications work partly by slowing gastric emptying.
For people with IBS, this can have unpredictable effects.
Further, for anyone with IBS, the most common GLP-1 side effects, including nausea, bloating, and abdominal discomfort, can overlap with and be difficult to distinguish from an IBS flare. [14]
The key distinction is timing: GLP-1 side effects tend to be most prominent when starting the medication or after a dose increase and typically ease over a few weeks as the body adjusts.
True IBS flares are more closely tied to food triggers, stress, or hormonal changes.
Current evidence does not suggest that GLP-1 medications worsen the underlying IBS condition itself.
If you have IBS and are taking or considering a GLP-1 medication, tracking symptoms carefully and working closely with both your prescribing physician and a gastroenterologist is important for managing both sets of symptoms effectively.
lf You Are Currently Taking Ozempic or Another GLP-1 Medication
Do not stop taking your GLP-1 medication due to gastrointestinal symptoms without first consulting your prescribing physician. Stopping abruptly can have health consequences, particularly for people managing type 2 diabetes. GI side effects from GLP-1 drugs (nausea, bloating, constipation, or diarrhea) are common, especially when starting or increasing your dose, and often improve with time. If you have IBS and are concerned about how your medication is affecting your symptoms, ask your doctor for a referral to a gastroenterologist who can help you manage both conditions together. The information in this section reflects the current available evidence and is not a substitute for personalised medical guidance.
IBS is diagnosed based on symptoms using the Rome IV criteria, but a healthcare provider must first rule out other conditions. See a doctor promptly if you experience any of the following:
These are recognized "red flag" symptoms by bodies including the American College of Gastroenterology and the UK's NICE guidelines, and they require clinical investigation to exclude more serious causes. [12]
Short-term: a heat pack on the abdomen, enteric-coated peppermint oil capsules, over-the-counter antispasmodics, and gentle movement such as walking. Long-term, the most effective approaches combine dietary changes like the low-FODMAP diet, regular exercise, consistent sleep, and stress management techniques such as cognitive behavioral therapy or gut-directed hypnotherapy.
IBS stools vary by subtype. In IBS-C, stools are hard and difficult to pass (Types 1 to 2 on the Bristol Stool Chart). In IBS-D, they are soft, mushy, or watery (Types 5 to 7). In IBS-M, both can occur, sometimes on the same day. IBS stools should not contain blood. If you notice rectal bleeding, see a doctor.
Use heat on the abdomen, try peppermint oil capsules, and take an antispasmodic for cramping. For IBS-D flares, loperamide can reduce urgency. Avoid known food triggers, keep meals small and plain, and reduce stress where possible. If flares are frequent or severe, or accompanied by red flag symptoms, speak with your doctor about prescription options.
The most common triggers include high-FODMAP foods such as onions, garlic, wheat, beans, certain fruits, and dairy; fatty or fried foods; caffeine; alcohol; carbonated drinks; and artificial sweeteners like sorbitol. Triggers are highly individual. A food and symptom diary, ideally with dietitian support, is the best way to identify your personal patterns.
Stress is the most consistently reported trigger for IBS flare-ups across clinical research. The gut-brain connection means that psychological stress directly alters gut motility and pain sensitivity through the hypothalamic-pituitary-adrenal axis, often causing or worsening symptoms in real time.
Several conditions commonly mimic IBS in women: endometriosis (which causes GI symptoms in over 75 percent of those affected), SIBO, celiac disease, pelvic floor dysfunction, ovarian cysts or cancer, and inflammatory bowel disease. A thorough medical evaluation, including blood tests and a review of symptom patterns, especially any cyclical worsening around menstruation, is needed to rule these out.
GLP-1 medications like Ozempic slow gastric emptying, which can cause nausea, bloating, and abdominal discomfort that resembles or overlaps with an IBS flare. For those with IBS-C, the slowed motility may worsen constipation. Current evidence suggests these medications do not worsen the underlying IBS condition, but their side effects can be difficult to distinguish from IBS symptoms. Side effects generally improve with time and dose adjustment. Careful symptom tracking and close collaboration with your medical team are recommended.
Medical Disclaimer
This article is intended for general informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. The information presented here is based on published research and expert commentary available at the time of writing and is not a substitute for a consultation with a qualified healthcare professional. IBS and the conditions discussed in this article are complex and present differently in each person. Treatment decisions, including dietary changes, medications, and gut-brain therapies, should always be made in partnership with a licensed gastroenterologist, physician, or registered dietitian who can assess your individual circumstances. If you are experiencing symptoms that concern you, please seek medical attention. Do not delay or disregard professional medical advice based on anything you have read in this article. Medication information is current as of the publication date and may change. Always verify prescribing information with your healthcare provider or pharmacist.
[2] Sex-Gender Differences in Irritable Bowel Syndrome. PMC/NIH, World Journal of Gastroenterology.
[6] Lee M, MD. What Women Should Know About IBS. Weill Cornell Medicine.
[7] Moza D, MD. Treating IBS in Women. Rochester Regional Health.
[9] Pimentel M. Menopause, HRT and the Gut Microbiome. National Geographic, May 2025.
[10] Palsson OS, Whitehead WE. Hormones and IBS. UNC Center for Functional GI and Motility Disorders.
[12] Irritable Bowel Syndrome (IBS). Cleveland Clinic.
[13] Hong-Curtis JA, MD. Why Gastrointestinal Problems Often Affect Women Differently. Yale Medicine.
[14] Ozempic with IBS/IBD: Distinguishing Flares from GLP-1 Side Effects. Polar Bear Meds.
[15] Irritable Bowel Syndrome: Symptoms and Causes. Mayo Clinic.
Estimated reading time: 10 minutes
| QUICK ANSWER: Noom uses CBT-informed behavioral coaching and suits people who want to understand the psychology behind their habits. Weight Watchers uses a point-based nutrition tracking system and is better for those who prefer community accountability. WW is more affordable; Noom offers more individualized coaching. Both now offer optional GLP-1 medication support via clinical tiers. |
| NOOM | WEIGHT WATCHERS | |
| Core Approach | Psychology & behavior change (CBT-inspired) | Point-based nutrition tracking |
| Food System | Color-coded (Green / Yellow / Orange) | ZeroPoint + daily points budget |
| Coaching | Dedicated 1:1 goal coach | Group coaches + workshops |
| Platform | App only | App + in-person hybrid option |
| Free Trial | Up to 14 days | Up to 30 days |
| Starting Price | ~$70/month; ~$17/month (annual) | ~$23/month |
| GLP-1 Medication | Available via Noom Med (Rx only) | Available via clinical tier (Rx only) |
| App Rating (iOS) | 4.7/5 | 4.8/5 |
| App Rating (Android) | 4.3/5 | 4.6/5 |
| Best For | Behavioral coaching, 1:1 support | Community support, food tracking |
Noom is a digital-only weight loss program built around behavior change.
Rather than prescribing a specific diet, Noom uses psychoeducational content drawn from behavioral science, including concepts from Cognitive Behavioral Therapy (CBT), to help you understand and modify the habits and thought patterns that may be contributing to weight gain.
It is important to note that Noom's coaching is not clinical CBT therapy.
The app delivers CBT-inspired lessons, prompts, and group support, but these are educational tools.
It is not a replacement for working with a licensed mental health professional.
Noom categorizes foods into three groups based on calorie and nutrient density:
Noom does not assign specific calorie counts to every food. Instead, the color system is designed to guide portion awareness without strict calorie counting.
Every Noom subscriber is assigned a coach who provides regular check-ins, motivation, and accountability.
This is one of Noom's key differentiators.
Group coaching and peer communities are also available within the app.
| Noom Service | Estimated Cost |
| Noom Weight Behavior change program with psychology-based lessons, habit tracking, and optional coaching. | $17.42/month with a 12-month plan (7 day trial available) |
| Noom GLP-1Rx Program Personalized GLP-1 treatment plan with SmartDose titration, coaching, and lifestyle support. | Starting at $129 |
| Noom Microdose GLP-1Rx Program Personalized GLP-1 plan designed to minimize side effects, and includes medication and 1:1 coaching. | Starting at $99 |
| Noom Proactive Health Microdose GLP-1Rx Program (New) Noom’s lowest-dose GLP-1 program to minimize side effects. Includes an easy at-home biomarker test kit. | $149/month |
| Noom Med: Telehealth for branded meds Combines weight-loss medication solutions with Noom’s psychological support. | $69 to get started |
| Noom HRTRx A menopause-focused program offering access to HRT, clinical guidance, and weight and symptom management. | $69 to get started |
Pricing is subject to change; always verify current rates at noom.com.
| Pros | Cons |
| ✓ Dedicated 1:1 human coaching | ✗ More expensive than WW, especially month-to-month |
| ✓ Behavioral focus addresses root causes of overeating | ✗ App-only; no in-person community option |
| ✓ No foods are forbidden; flexible approach | ✗ Limited structured nutritional guidance |
| ✓ Flexible subscription options | ✗ Daily lessons require consistent engagement |
| ✓ GLP-1 medication available via Noom Med | ✗ CBT-inspired content is not clinical therapy |
Weight Watchers, now officially rebranded as WW, was founded in 1963 and is one of the most established commercial weight loss programs in the world.
Rather than focusing on calorie counts, WW assigns each food a point value (called PersonalPoints) based on its calorie, protein, sugar, and saturated fat content.
You receive a personalized daily points budget and build your meals within it.
A defining feature of WW is its ZeroPoint foods list, items that carry no point value and can be eaten freely.
These include non-starchy vegetables, most fruits, lean proteins like chicken breast and fish, eggs, and legumes.
The goal is to make healthy eating the easy default, without requiring you to meticulously count every bite.
WW's strongest differentiator is its community infrastructure.
Members can attend virtual or in-person workshops led by trained WW coaches, connect with a peer community, and access one-on-one coaching.
The in-person option sets WW apart from Noom for people who find face-to-face accountability motivating.
Weight Watchers has three main membership tiers in 2026, all based on a 12-month commitment that auto-renews:
| Program | What It Is | Price |
| Core Program | A customized food plan and an easy to-use app with science-backed tools for lasting weight loss | Starts at $10/month |
| Core+ | A customized food plan + app access + community support | Starts at $20/month |
| Core+ Menopause | Access to HRTs, GLP1s, menopause-focused weight loss programs, expert medical support, etc | May start at ~$88/month* |
| GLP-1 success | Nutrition and fitness programs to reduce side effects and maximize efficacy of GLP-1 drugs (drugs not included) | Starts at $20/month |
| Med+ | Access to GLP-1s and other weight-loss medications along with clinician support | $25, then $74/month for the remainder of a 12-month plan Cost of GLP-1 meds not included |
Approximate cost of medicaitons
| Pros | Cons |
| ✓ More affordable entry price | ✗ Point tracking can be tedious in real-world scenarios |
| ✓ Strong community & in-person workshop option | ✗ Weekly weigh-ins may be problematic for some individuals |
| ✓ No foods are off-limits | ✗ Less personalized than Noom's 1:1 coaching model |
| ✓ Flexible digital or hybrid memberships | ✗ Community quality may vary by location |
| ✓ Longer track record and evidence base | ✗ Point system can feel restrictive for some eating styles |
GLP-1 receptor agonists (such as semaglutide and tirzepatide) are prescription-only medications. Noom now offers four distinct clinical pathways: (1) Noom Microdose GLP-1Rx from $99, designed for lower doses to reduce side effects; (2) Noom GLP-1Rx Program — from $119, with SmartDose titration and coaching; (3) Noom GLP-1Rx Plus (tirzepatide) — from $199; and (4) Noom Med telehealth for branded medications (Ozempic, Wegovy, Zepbound, Mounjaro, Liraglutide) from $69 (medication cost separate). All require medical consultation and eligibility assessment. Compounded medications available through Noom are not FDA-reviewed for safety, efficacy, or quality. Always consult a licensed healthcare provider.
Noom has significantly expanded its clinical offerings.
A key addition is the GLP-1 Companion, a free add-on included with Noom Weight for users already taking GLP-1 medications, featuring protein tracking, Muscle Defense workouts, and side-effect management guides.
Noom also now offers a Proactive Health Microdose GLP-1Rx Program at $149/month (medication included) targeting metabolic health and biomarker improvement, and a Noom HRTRx program for menopause-related hormone therapy.
These are prescription-only and require medical consultation.
Noom has faced criticism from some healthcare providers and user groups who argue that the app's emphasis on food color-coding, daily weigh-ins, and caloric awareness may be triggering or harmful for individuals with a history of disordered eating.
While Noom positions itself as an anti-diet program, critics note that the mechanics of food tracking and weight monitoring are consistent with dietary restraint models associated with eating disorder risk in vulnerable populations.
Noom has responded to this criticism by adding eating disorder screening questions during onboarding and providing clinical escalation pathways. However, the academic evidence on this specific risk is limited, and clinical guidance varies.
If you have a current or past history of an eating disorder, please consult a healthcare provider or registered dietitian before starting Noom or any structured weight loss program. Support is available via the National Alliance for Eating Disorders.
| Factor | NOOM | WW |
| Philosophy | Behavior & psychology first (CBT-inspired) | Nutrition & food tracking first |
| Structure | Flexible; color guidance, not strict tracking | More structured; daily points must be tracked |
| Coaching model | 1:1 goal coach + AI support in-app | Group workshop coaches |
| In-person option | No (app only) | Yes (hybrid plans) |
| Price (Core/digital) | $42.25/month (4-month plan) | $23/month standard; promo from $10/mo |
| Price (committed plan) | $17.42/month (12-month, $209 upfront) | $10/month (10-month promo plan) |
| Price (clinical/GLP-1) | Microdose from $99; GLP-1Rx from $119 (med included) | Med+ Clinic: $25 first mo, then $74/mo; medication separate |
| New programs (2025–26) | Microdose GLP-1, GLP-1 Plus (tirzepatide), Proactive Health, HRTRx, Body Scan, Muscle Defense | Clinical GLP-1 tier; community workshops |
Choose NOOM if: You want to understand the behavioral and psychological roots of your eating habits, prefer personalized 1:1 coaching, and are comfortable with app-based daily engagement. Noom is particularly well-suited to people who have tried nutrition-focused diets without long-term success and suspect that mindset or habit patterns are part of the picture.
Choose WEIGHT WATCHERS if: You do better with community accountability, prefer a structured food tracking method, and want the option to attend in-person or virtual workshops. The Core plan is among the most affordable entry points in structured weight loss ($10/month on promotional 10-month plans). If you are already on or considering GLP-1 medication, the Med+ Clinic tier provides telehealth access to prescribers, though note the medication cost is billed separately and the plan requires a 12-month commitment.
Both programs are legitimate, evidence-supported tools for weight management, but neither is a one-size-fits-all solution. The best program is the one you will actually stick with. Consider starting with the free trial period of each before committing to a subscription.
Both have supporting clinical evidence for short-term weight loss outcomes. Noom's behavioral approach may offer an advantage for individuals who have struggled with habit-driven overeating. WW's community model has demonstrated sustained engagement over decades. Long-term success with either program depends significantly on individual adherence and personal fit.
Noom Weight: $17.42/month (12-month plan, $209 upfront); $29.83/month (6-month); $42.25/month (4-month). GLP-1 clinical programs from $99–$199+ (medication included for compounded options). WW Core (digital): $23/month standard, or as low as $10/month on a promotional 10-month plan. WW Med+ Clinic (GLP-1 telehealth): from $25 first month, then $74/month (medication billed separately). Prices verified March 2026; always confirm at noom.com and weightwatchers.com.
Yes. Both offer GLP-1 medication access through their respective clinical tiers (Noom Med; WW clinical membership). These medications are prescription-only and require a medical consultation. They are not appropriate for everyone.
Noom has faced criticism in this area. Its calorie-awareness tools and weigh-in features may be triggering for some users. If you have a history of disordered eating, consult a healthcare provider before starting any structured weight loss program.
WW offers in-person workshops through its hybrid membership plans. Noom is app-only and does not have a physical presence. If in-person support matters to you, WW is the better option.
1. Painter SL et al. (2017). What Matters in Weight Loss? An In-Depth Analysis of Self-Monitoring. J Med Internet Res. PMC 4446719.
2. Noom weight loss app efficacy review (2023). PMID 36621904.
3. Garage Gym Reviews: Noom vs Weight Watchers Comparison. garagegymreviews.com
4. Weight Watchers official comparison page. weightwatchers.com
5. Medical News Today: Noom vs Weight Watchers. medicalnewstoday.com
6. Second Nature US: Noom vs Weight Watchers. secondnature.io
Estimated reading time: 17 minutes
Melatonin is a hormone.
The body produces it naturally to regulate the sleep-wake cycle, also called the circadian rhythm.
Levels typically rise in the evening, peak during the night, and fall toward morning.
As a supplement, melatonin is available over the counter in most countries.
It is not a sedative. It does not force sleep. It signals to the body that it is time to wind down.
Melatonin is primarily produced in the pineal gland, a small pea-sized structure located deep in the brain.
Production is triggered by darkness and suppressed by light, which is why light exposure at night can interfere with sleep.
The retina, gut, and skin also produce small amounts of melatonin, though the pineal gland accounts for the majority of what enters the bloodstream.
Research published in the Journal of Pineal Research confirms that light-induced suppression of pineal melatonin is one of the primary mechanisms disrupting modern sleep patterns[1].
Melatonin supplements work by mimicking the body's natural signal for sleep onset.
They shift the body's internal clock, making them most useful for circadian rhythm-related issues such as jet lag[2], shift work[3], or delayed sleep phase disorder[4].
For general insomnia, the evidence is more modest.
A 2013 meta-analysis in PLOS ONE found that melatonin reduced sleep onset latency by an average of about 7 minutes[5]. That is meaningful for some people, less so for others.
Most formulations of melatonin begin to take effect within 30 to 60 minutes.
Peak blood concentration is typically reached within 1 to 2 hours after ingestion, depending on the formulation (immediate-release versus extended-release) and individual metabolism.
Genetic variation in CYP1A2, an enzyme involved in melatonin breakdown, can affect how quickly the body processes it[6].
Some individuals clear melatonin faster, which may shorten its window of effectiveness.
Supplement doses in the US commonly range from 1 mg to 10 mg, but research suggests the effective dose is much lower for most people[7].
A 2001 study by MIT researchers, published in Sleep, found that doses as low as 0.3 mg were effective at raising blood melatonin levels to physiological levels[8].
Higher doses produce supraphysiological levels, far above what the body naturally produces, without a proportional increase in benefit.
10 mg is significantly above the dose supported by most research[9]. Studies have not established that 10 mg of melatonin produces better sleep outcomes than lower doses.
What higher doses do produce is a longer duration of elevated melatonin in the blood, which may contribute to morning grogginess, headaches, or mood changes the following day.
Taking it every night without medical guidance is not recommended.
These two sleep aids work through entirely different mechanisms.
Ambien (zolpidem) is a sedative-hypnotic that acts on GABA receptors in the brain[10]. Melatonin is a hormone that signals circadian timing.
There is no equivalence in terms of sedative potency.
Melatonin is appropriate for circadian rhythm disruptions. Ambien is prescribed for more acute insomnia.
Attempting to use melatonin as a direct substitute for a prescription sleep aid may not address the underlying issue.
Melatonin not working is a common complaint.
The explanation is often one of three things: incorrect timing, too high a dose, or a sleep issue for which melatonin is not the right tool.
Melatonin is most effective for circadian rhythm issues, not for all sleep problems. If the underlying issue is anxiety, pain, sleep apnea, or stress, melatonin is unlikely to help significantly.
Timing also matters. Taking melatonin too late, after the body has already begun its natural melatonin surge, may produce little additional effect.
Research suggests taking it 30 to 45 minutes before the desired sleep onset.
Individual variation is also a factor.
Genetic differences in melatonin receptor sensitivity (MTNR1A and MTNR1B gene variants)[11] and in melatonin metabolism (CYP1A2) can influence how a person responds.
What works at 1 mg for one person may require a different dose or timing for another.
Melatonin is generally considered low-risk for interactions, but it is not entirely without them. Below are the most common combination questions.
NyQuil contains antihistamines (diphenhydramine or doxylamine) and often acetaminophen.
Both antihistamines and melatonin have sedative properties. Taking them together may amplify drowsiness.
NyQuil versions with alcohol add another layer of concern.
Central nervous system depression from multiple sedating agents can be unpredictable. This combination is best avoided without medical guidance.
There is no established harmful interaction between magnesium and melatonin. Some sleep supplements combine both.
The mechanisms are different enough that they can complement each other: melatonin for circadian signaling, magnesium for nervous system regulation.
Starting with lower doses of each and monitoring response is a reasonable approach.
There is no well-documented pharmacokinetic interaction between acetaminophen (Tylenol) and melatonin at standard doses[12]. They are processed through different pathways.
However, both can affect the liver in high doses or with chronic use. Taking either within normal recommended limits is generally considered safe for healthy adults. If there is an existing liver concern, a doctor should be consulted.
This combination is not recommended. Alcohol is a CNS depressant.
Melatonin, though not a sedative, also has CNS-modulating effects.
Together, they can increase drowsiness in an unpredictable way and may disrupt sleep, particularly REM sleep, more than alcohol alone[13].
Alcohol already suppresses melatonin production, according to research published in the Journal of Clinical Endocrinology and Metabolism[14].
Adding a supplement on top of that disruption does not clearly restore normal sleep quality.
| Expert picks: What To Read Next |
|---|
| What Is The Best Sleeping Position For Lower Back Pain? |
| The Top 3 Methods To Fall Asleep Faster |
| Why Do I Keep Waking Up At 4 AM |
The body produces melatonin endogenously, but certain foods also contain it in measurable amounts.
Dietary melatonin is unlikely to match supplement doses, but may support natural melatonin activity[15].
Yes. Both grapes and kiwi contain melatonin.
A 2011 study in the Journal of Pineal Research found that melatonin was present in various grape varieties, with the skin containing higher concentrations[16].
Kiwi has been studied for its effects on sleep.
A 2011 study in the Asia Pacific Journal of Clinical Nutrition found that eating 2 kiwifruits 1 hour before bedtime for 4 weeks was associated with improved sleep onset and duration[17].
Whether melatonin specifically or other compounds in kiwi were responsible for the effect remains under investigation.
Tart cherries are among the most studied dietary sources of melatonin.
A 2012 study in the European Journal of Nutrition found that Montmorency tart cherry juice increased urinary melatonin levels and was associated with modest improvements in sleep duration and quality[18].
Melatonin content varies across cherry types, with tart varieties generally containing higher concentrations than sweet cherries.
Pistachios contain melatonin in comparatively high amounts relative to other foods.
A research article published in the Journal of Clinical Research and Reports mentions that melatonin is present in pistachio nuts[19].
But the amount found is 500-1000 times lower than that found in medicinal products or supplements containing melatonin, and therefore cannot exert any biological effects.
Short-term use, days to a few weeks, is generally considered safe for most healthy adults.
Long-term nightly use is less studied, which makes it harder to give a confident answer about extended daily use[20].
Most research suggests taking melatonin 30 to 45 minutes before the intended sleep time.
For circadian phase shifting, such as adjusting to a new time zone, some protocols recommend taking it even earlier, 1 to 2 hours before target bedtime.
Timing is arguably more important than dose for melatonin to work as intended.
Melatonin does not appear to be addictive in the pharmacological sense.
It does not bind to receptors associated with dependence, and withdrawal symptoms have not been documented in the clinical literature[21].
The difficulty of sleeping without it is possible for any sleep aid over time, including non-addictive ones.
Sleep hygiene practices, along with supplementation, may reduce this risk.
Yes. Like all supplements, melatonin degrades over time. Expired melatonin may be less potent, but it is not typically considered dangerous.
Storing supplements in a cool, dry place away from light extends shelf life.
Most melatonin supplements have expiration dates of 1 to 3 years from the date of manufacture.
Using a product past its expiry date is not recommended, primarily because its efficacy is reduced.
The honest answer is that long-term safety data on nightly melatonin use in healthy adults is limited.
Short-term use across weeks to a few months has a reasonably established safety profile.
One concern raised, primarily in animal studies, is whether exogenous melatonin could suppress the body's endogenous production over time.
Evidence in humans for this is not conclusive.
Studies have noted that melatonin has a favorable short-term safety profile, but called for more long-term human trials[22].
Melatonin is generally well tolerated. Most people who take it at appropriate doses report no side effects at all[23].
When side effects do occur, they tend to be mild, short-lived, and dose-dependent.
They are more commonly higher doses which is another reason researchers suggest starting low.
The most commonly reported side effects include:
Less frequently, some people report mood changes, irritability, or gastrointestinal discomfort such as diarrhea or constipation.
The sections below address each of these in more detail.
Research indicates that melatonin promotes the release of vasotocin, a substance linked to memory processing during REM sleep[24].
Vasotocin helps the brain erase certain memories while you dream, allowing for clear differentiation between dreams and reality upon waking.
Supplemental melatonin can increase vasotocin levels, potentially extending or intensifying REM sleep periods.
This enhanced REM activity often leads to more vivid and intense dreams, which some people may interpret as nightmares.
In some cases, the changes melatonin causes in the sleep cycle can disrupt normal brain processes related to dream regulation, triggering more frightening or disturbing dream content.
Overall, while melatonin supplements generally improve sleep quality, their influence on REM sleep and memory-related brain chemicals can lead to vivid or unsettling dreams in susceptible individuals.
More research is needed to fully understand the mechanisms behind melatonin-induced nightmares.
Headache is one of the more commonly reported side effects in clinical studies[25].
If headaches occur consistently after taking melatonin, reducing the dose or discontinuing use is a reasonable step.
Melatonin is more often studied as a potential anxiolytic, meaning it may reduce anxiety in some contexts, particularly preoperative anxiety, according to several small clinical trials[26].
That said, some individuals report feeling more anxious or restless after taking it.
Gastrointestinal complaints, including nausea, diarrhea, and constipation, are occasionally reported.
The gut contains melatonin receptors, and melatonin plays a role in gastrointestinal motility, which may explain why some people experience GI effects[27].
There is no strong evidence that melatonin at standard supplement doses causes weight gain in humans.
Some research, primarily animal studies, has explored melatonin's role in metabolic regulation and fat distribution, but the direction of effects is complex and not consistently translated to humans[28].
A 2012 study in the Journal of Pineal Research found melatonin associated with reduced adiposity in certain animal models, suggesting the relationship is not straightforward[29].
Sleep isn't just about your circadian rhythm. Your nutrition affects melatonin production. Caffeine metabolism impacts sleep quality. Underlying health risks like diabetes and heart disease disrupt rest. The Xcode Life Genome Pack analyzes all interconnected factors and health risks, so you can finally understand and fix your sleep issues from every angle.
Some questions about melatonin touch on more significant health concerns. The research on most of these is either reassuring or still emerging.
The relationship between melatonin and heart health is an area of emerging concern.
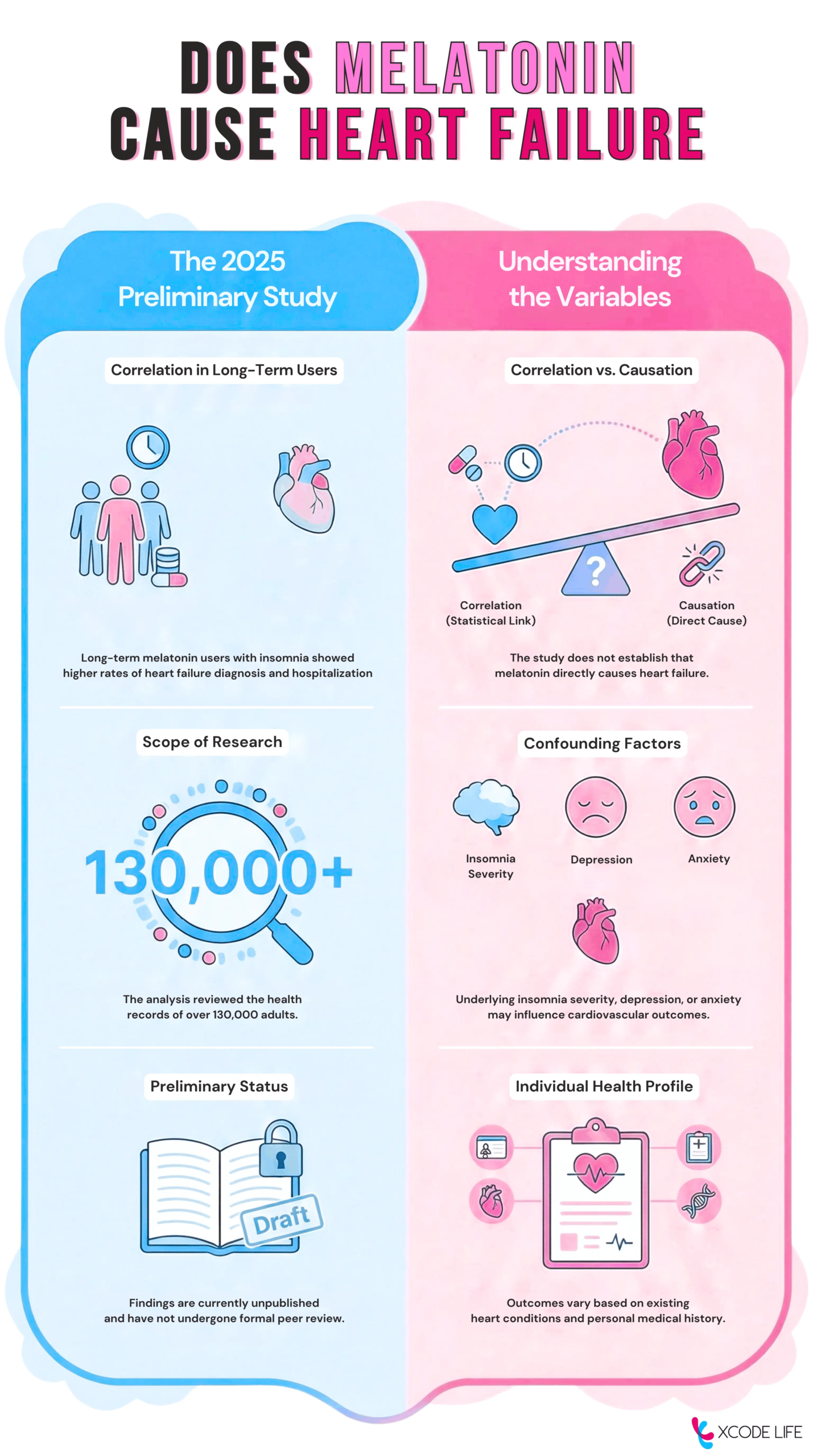
A 2025 preliminary study presented at the American Heart Association's Scientific Sessions, which reviewed health records of over 130,000 adults with insomnia, found that long-term melatonin users had a significantly higher rate of heart failure diagnosis and hospitalization compared to non-users[30].
However, the study has important limitations. It has not yet been peer-reviewed or published in a full scientific journal.
It also could not establish cause and effect.
It is possible that the underlying severity of insomnia, or related conditions such as depression and anxiety, contributed to both melatonin use and cardiovascular risk.
The researchers themselves noted that more research is needed.
People with existing heart conditions should discuss melatonin use with their cardiologist. For otherwise healthy adults, this study warrants attention but does not yet constitute definitive evidence of harm.
Research indicates melatonin may have a modest blood pressure-lowering effect.
A 2019 meta-analysis of randomized controlled trials published in the Journal of Hormone and Metabolic Research found statistically significant reductions in both systolic and diastolic blood pressure with melatonin supplementation[31].
However, subsequent analyses suggest this effect may be specific to controlled-release formulations; standard fast-release supplements appear to have little impact on blood pressure.
For most healthy individuals, this effect is unlikely to be clinically significant. For people taking antihypertensives, the combination could theoretically enhance blood pressure reduction[32] and warrants medical supervision.
There is no established evidence that melatonin causes dementia.
The relationship, where it exists in the research, tends to go in the opposite direction[33].
Melatonin levels naturally decline with age, and some studies have explored whether this decline is linked to increased dementia risk.
Research in Frontiers in Aging Neuroscience has examined melatonin's neuroprotective potential, though this remains an area of active study[34]. No current evidence indicates supplemental melatonin is harmful to cognitive health.
For most healthy adults, melatonin taken at appropriate doses and for appropriate durations is not harmful. The key qualifiers are dose (lower is generally better), duration (short-term use has more established safety data), and individual health context.
It is worth noting that melatonin supplements are not regulated with the same rigor as prescription drugs. Independent testing has shown significant variation between labeled and actual melatonin content across products.
A 2017 study in the Journal of Clinical Sleep Medicine found that actual melatonin content varied from -83% to 478% above the stated amount[35].
Melatonin has a wide safety margin.
Documented cases of serious toxicity from melatonin overdose are extremely rare.
That said, taking more than necessary is not without consequences.
Symptoms of taking too much melatonin can include excessive drowsiness, headache, nausea, dizziness, and irritability.
These tend to be self-limiting and resolve as the supplement clears the system.
More significantly, very high doses can disrupt the circadian rhythm rather than support it, effectively defeating the purpose of taking melatonin in the first place.
A life-threatening overdose from melatonin gummies specifically has not been well-documented in adults.
However, gummies present a practical risk, particularly for children, because they are palatable and easy to consume in excess.
Poison Control data in the US has recorded a significant increase in pediatric melatonin ingestion incidents in recent years.
A 2022 report in Pediatrics documented over 260,000 pediatric melatonin ingestion cases between 2012 and 2021, with hospitalizations increasing in more recent years[36].
Gummies should be stored out of reach of children.
Melatonin is not appropriate for everyone at standard supplement doses. Certain populations require more caution.
For most healthy adults using melatonin short-term and at low doses, the risk profile is generally considered acceptable.
But "generally safe" is not the same as "safe for everyone." Age, hormonal status, underlying health conditions, and concurrent medications can all influence how melatonin behaves in the body.
Because it interacts with the endocrine system, populations with developing or hormonally sensitive physiology, such as children and adolescents and those who are pregnant, warrant particular consideration. The sections below cover the groups where caution is most warranted based on available evidence.
There is insufficient human research on melatonin supplementation during pregnancy to establish safety.
Melatonin crosses the placenta and may influence fetal circadian development.
Animal studies suggest melatonin plays a role in fetal programming, though the implications for human supplementation are not well understood[37].
Most healthcare guidelines recommend avoiding melatonin supplements during pregnancy unless specifically advised by an obstetrician.
Pediatric melatonin use has increased significantly over the past decade, but it is not approved for children by the FDA in the US, and the long-term effects on the developing endocrine system are not fully established[38].
Short-term use in children with specific conditions such as autism spectrum disorder or ADHD, where sleep disturbances are common, has been studied with generally positive short-term outcomes[39].
The American Academy of Sleep Medicine suggests that behavioral sleep interventions should be tried first. If melatonin is considered, it should be under pediatric supervision with the lowest effective dose[40].
Pet owners frequently search melatonin questions for their animals. The answers here differ from human guidance.
Melatonin is used in veterinary practice for dogs, primarily for anxiety, noise phobias, and certain hormonal conditions[41].
It is generally considered safe for dogs at appropriate doses, which are body-weight dependent.
The critical warning: many human melatonin supplements, particularly gummies, contain xylitol as a sweetener. Xylitol is toxic to dogs and can cause severe hypoglycemia[42].
Any melatonin given to a dog must be xylitol-free. A veterinarian should be consulted before use.
Melatonin use in cats is less studied than in dogs. Some veterinarians use it off-label for anxiety and sleep regulation.
However, cats metabolize many compounds differently from humans and dogs, and there is less clinical data available.
Melatonin should not be given to cats without veterinary guidance.
The dose, formulation, and appropriateness for the individual animal's health status all require professional evaluation.
Melatonin is one of the most widely used supplements in the world, and for good reason. It is generally well tolerated, accessible, and supported by evidence for specific uses such as jet lag and circadian disruption.
But it is not a universal sleep fix, and it is not without nuance. Dose matters more than most people realize.
Individual biology, including genetic variation in how melatonin is metabolized and how sensitive a person's receptors are, means that what works well for one person may do little for another.
If melatonin has not worked for you, or if you have questions about whether it is appropriate for your health situation, a conversation with a healthcare provider is the most reliable next step.
Estimated reading time: 6 minutes
Insomnia (also known as sleeplessness) is a common sleep disorder that is characterized by the inability to fall asleep or stay asleep at night, resulting in tired or unrefreshing sleep.
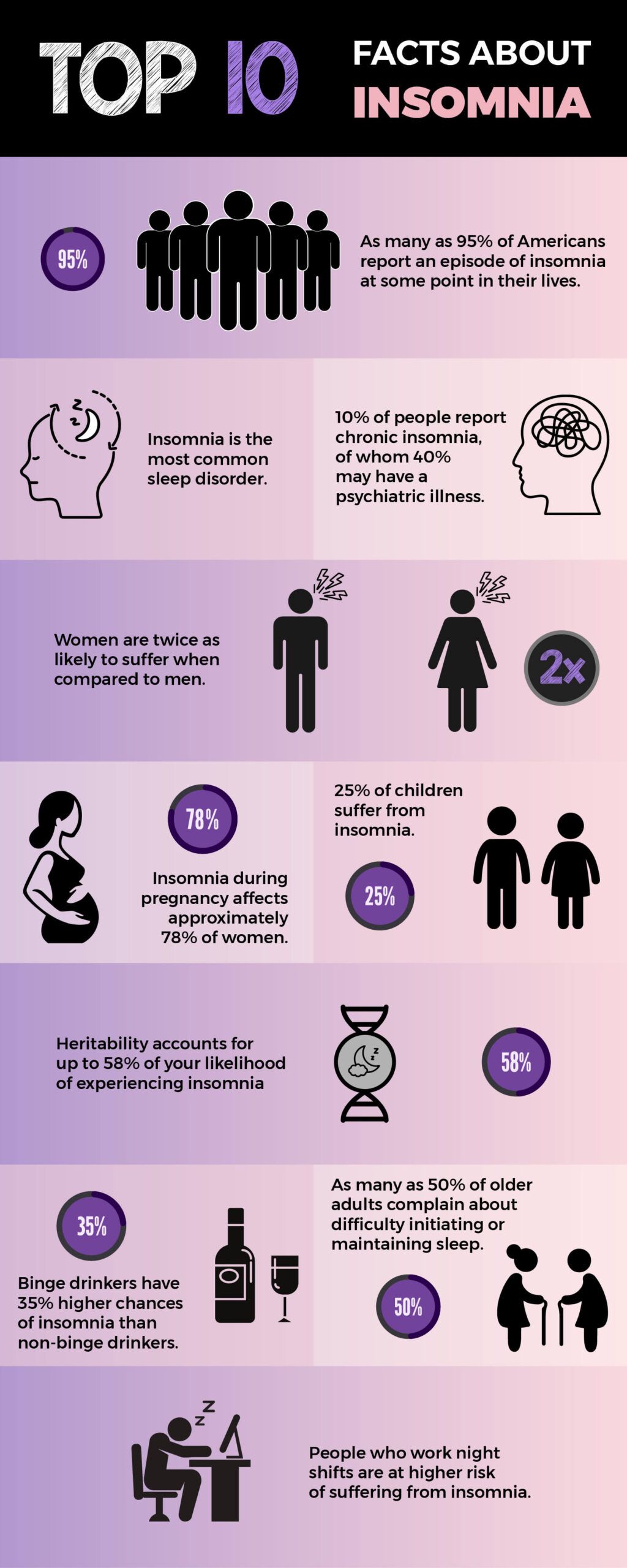
According to the American Psychiatric Association (APA), insomnia is the most common sleeping disorder.
Research indicates that approximately 10% of adults worldwide meet the criteria for chronic insomnia.
Approximately 30% to 40% of adults in the United States report occasional symptoms of insomnia.
A diagnosis of insomnia needs to meet the following two categories:
This can be caused by variations in biological, psychological, and social factors, which most often result in a reduced amount of sleep.
People with parents or siblings with insomnia have an increased risk of experiencing the condition themselves. This indicates a genetic link to insomnia.
This was further confirmed by a 2018 study that reported that insomnia has a partially heritable basis. In fact, heritability accounts for 31% to 58% of your insomnia risk.
Insomnia also appears to share genetic links with other health conditions.
The researchers also found a strong genetic link between insomnia and type 2 diabetes.
Tissue-specific gene-set analyses showed that insomnia might have higher genetic signals among genes that are usually expressed in the brain.
The functions of these regions of the brain are of relevance to insomnia.
The genetic correlations between insomnia and psychiatric traits were stronger than the genetic correlations between insomnia and other sleep-based characteristics.
The study suggests that, genetically, insomnia resembles neuropsychiatric traits more closely than other sleep-related characteristics.
The MEIS1 gene is a transcription factor that plays a key role in hematopoiesis, endothelial cell development, and vascular patterning.
It also plays a role in neurodevelopment.
Research studies have shown that the reduced MEIS1 levels and function of the gene may contribute to the pathogenesis of sleep-related disorders.
The rs113851554 is a G>T polymorphism located in the MEIS1 gene, which is found to be correlated with multiple sleep disorders.
A study found that the T allele of rs113851554 is associated with an increased risk of developing insomnia symptoms.
Functional study analysis suggested that the rs113851554 in the MEIS1 locus is most strongly associated with insomnia disorder.
A 2026 review published in Frontiers in Medicine evaluated 105 Mendelian randomization studies.
This research indicates that genetic susceptibility to insomnia causally increases the risk of developing over 30 chronic conditions. These conditions include coronary heart disease, severe depression, and type 2 diabetes.
Additionally, integrative genomics research analyzing over 386,000 individuals identified 449 genes associated with insomnia risk. The study prioritized five promising genes: DALRD3, LDHA, HEBP2, TEX264, and FGFR3.
These genes may help explain the underlying biological mechanisms and altered brain functions involved in the disorder.
While these studies confirm a strong genetic link, insomnia genes are non-deterministic.
Individual sleep patterns vary greatly because genetic risk factors interact with environmental and lifestyle variables.
A genetic predisposition suggests susceptibility, but it does not guarantee an individual will develop clinical insomnia.
Upload your existing 23andMe or Ancestry DNA data to uncover sleep risks, nutrition factors affecting rest, and personalized solutions, all in one $199 report pack.
50,000 users globally. Rated 4.6/5
Insomnia is more common in women than in men.
More than one in four women in the United States experience insomnia, compared with fewer than one in five men.
Insomnia is more common in older people than in younger ones.
As many as 50% of older adults complain about difficulty initiating or maintaining sleep.
Medical and psychiatric conditions can increase insomnia risk.
Insomnia is more commonly seen in those with heart disease, asthma, depression, and anxiety than their healthier counterparts.
Yes, insomnia has a strong genetic component. Research indicates heritability accounts for 31–58% of an individual's risk though genes alone do not determine outcomes.
No, your severe lack of sleep is almost certainly common, treatable insomnia rather than the exceptionally rare genetic disease FFI.
No, while DNA tests can highlight natural genetic predispositions to sleep issues, they cannot medically diagnose the definitive root cause of your clinical insomnia.
Yes, a genetic susceptibility to insomnia directly increases your risk for developing conditions like type 2 diabetes, coronary heart disease, and depression.
Yes, you can absolutely overcome it; Cognitive Behavioral Therapy for Insomnia (CBT-I) is a highly effective, gold-standard treatment regardless of your genetic background.
Research suggests diet can influence insomnia symptoms. A 2024 meta-analysis of 591,223 individuals found high-quality diets linked to a 34% lower risk, while unhealthy dietary patterns raised risk by 20%.
CBT-I (Cognitive Behavioral Therapy for Insomnia) is the most evidence-based treatment for insomnia, carrying a strong recommendation in AASM guidelines.
https://pubmed.ncbi.nlm.nih.gov/30804565/
https://pubmed.ncbi.nlm.nih.gov/26132482/
| Expert picks: What To Read Next |
|---|
| What Is The Best Sleeping Position For Lower Back Pain? |
| Why Do I Keep Waking Up At 4 AM? |
Estimated reading time: 13 minutes
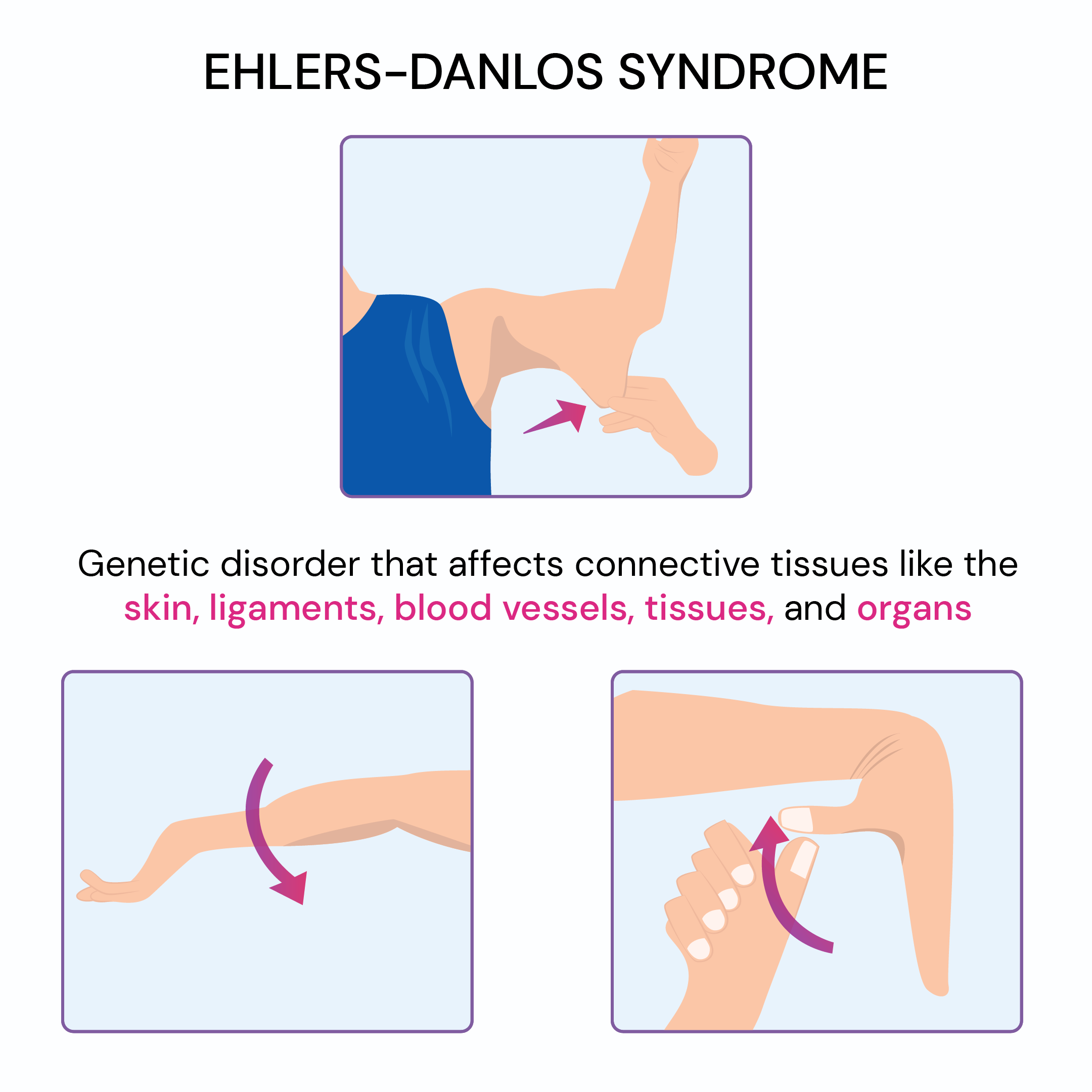
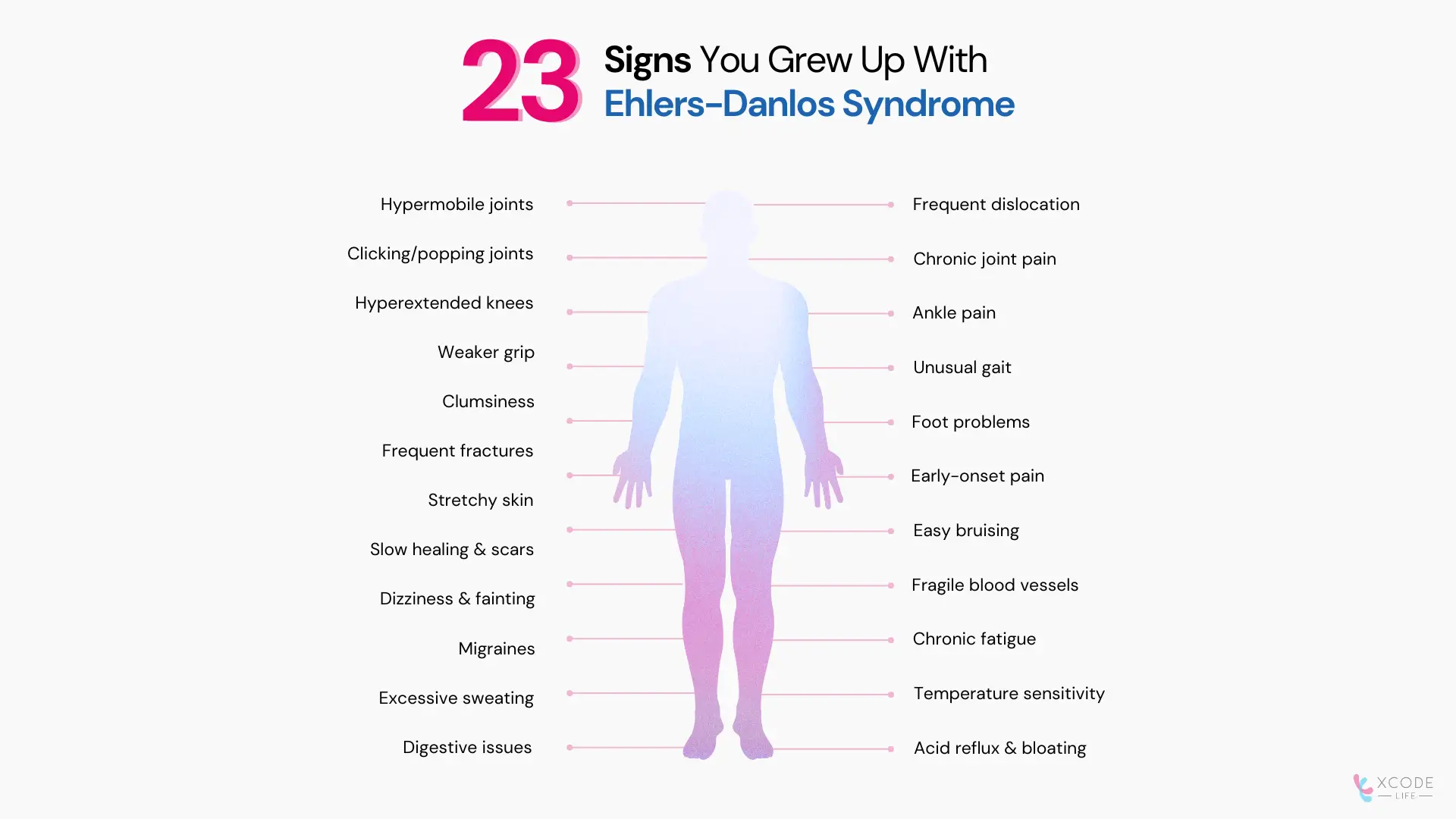
1. Hypermobile joints (double-jointed flexibility)
2. Frequent joint dislocations or subluxations
3. Clicking or popping joints
4. Chronic joint pain and instability
5. Hyperextended knees
6. Ankle pain during growth spurts
7. Weak grip strength (e.g., difficulty opening jars)
8. Clumsiness and uncoordinated movements
9. Frequent foot problems (flat feet, plantar fasciitis)
11. Chronic pain beginning at a young age
12. Soft, stretchy, or velvety skin
13. Easy bruising, often from minor contact
14. Slow wound healing and prominent or "cigarette paper" scars
15. Fragile blood vessels; prone to injury even under light pressure
17. Dizziness and fainting, often linked to POTS (postural orthostatic tachycardia syndrome) [1]
18. Chronic fatigue
19. Frequent migraines or chronic headaches
20. Sensitivity to temperature changes
21. Acid reflux and bloating
22. Nausea, constipation, or diarrhea (often linked to gastrointestinal dysmotility)
23. Bladder issues (urinary urgency or incontinence)
Note on Sign #23: Bladder and pelvic floor dysfunction are now recognized as common but frequently overlooked features of EDS, particularly in hypermobile EDS. Weak connective tissue in the pelvic floor contributes to these issues [2].
| Sign | Likely Cause | Notes |
| Hypermobile joints | Weak connective tissue | Core diagnostic sign across subtypes |
| Easy bruising | Fragile blood vessels | Appears even with minor trauma |
| Slow wound healing | Collagen defects | May leave "cigarette paper" scars |
| Dizziness/fainting | Autonomic dysfunction (POTS) | Common in hypermobile EDS |
| Digestive issues | Weak connective tissue in gut | Acid reflux, constipation, bloating |
| Chronic headaches | Dysautonomia, TMJ dysfunction, craniocervical instability | Can also reflect Chiari I malformation [3] |
| Bladder symptoms | Pelvic floor connective tissue weakness | Underdiagnosed; seen especially in women with hEDS [2] |
Dr. Blair Grubb, a cardiologist specializing in autonomic disorders at the University of Toledo Health
Sciences, highlights the systemic nature of EDS:
Research confirms this systemic view. A 2025 genome-wide association study (GWAS) meta-analysis of hEDS identified genetic correlations with myalgic encephalomyelitis/chronic fatigue syndrome, fibromyalgia, depression, anxiety, and autism spectrum disorder, confirming that EDS is fundamentally a multi-system condition [4].
*Asymptomatic hypermobility: A condition where a person's joints can move more than usual (are extra flexible), but they don't experience any pain or problems because of it.
**Autonomic test results: The outcomes from medical tests that check how well the body's automatic systems, like heart rate, blood pressure, and digestion, work.
There are 13 recognized subtypes of EDS [5], ranging from common to ultra-rare. Some of the main ones include:
Important update on prevalence: The traditional figure of "1 in 5,000 for all EDS" is increasingly recognized as an underestimate when subtypes are considered individually. The Ehlers-Danlos Society now emphasizes that hEDS may be far more common than 1 in 5,000 and that a single combined prevalence figure masks the dramatic variation across subtypes [6].
Yes, EDS is caused by variants in genes that produce collagen or the proteins that support connective tissue structure [7].
| Gene | Associated EDS Type | Function |
| COL5A1/COL5A2 | Classical EDS | Collagen type V production |
| COL3A1 | Vascular EDS | Collagen type Ill production |
| COLIA1/COLIA2 | Classical and rare types | Collagen type I production |
| TNXB | Classical-like EDS | Tenascin-X protein (supports connective tissue structure) |
| PLOD1 | Kyphoscoliotic EDS | Collagen crosslinking enzyme |
| KLK15 | Hypermobile EDS (some cases) | Kallikrein-15 protease; connective tissue and immune regulation |
| Expert picks: What To Read Next |
|---|
| Ehlers Danlos Syndrome And The Eyes |
| Which Parent Carries The Autism Gene? |
For many years, hEDS was the only EDS subtype without a known genetic cause. This made diagnosis rely entirely on clinical criteria and left patients without genetic confirmation of their conditions.
In June 2024, researchers from the Norris Lab at the Medical University of South Carolina published a landmark study identifying variants in the Kallikrein gene family, specifically a missense variant in KLK15 (p.Gly226Asp), as a likely cause of hEDS in some patients[8].
Key findings:
A separate 2025 GWAS meta-analysis (1,815 hEDS cases, 5,008 controls) identified two genome-wide significant loci, including a regulatory region near the ACKR3 gene (atypical chemokine receptor 3), implicating neuroimmune and pain signaling pathways in hEDS pathogenesis [4].
Already tested your DNA? Here’s how to use it further.
If you’ve tested with Ancestry, 23andMe, or similar services, your raw DNA file can be analyzed for deeper health insights.
EDS, Marfan syndrome, fibromyalgia, and joint hypermobility syndrome share overlapping symptoms, including joint hypermobility and chronic pain.
The 2017 international EDS classification also introduced a distinct category, Hypermobility Spectrum Disorder (HSD), for those who have symptomatic joint hypermobility but don't fully meet hEDS criteria. The boundary between hEDS and HSD remains clinically debated [12].
Accurate diagnosis requires detailed clinical evaluation and, where applicable, genetic testing.
There is currently no cure for EDS, but treatment helps manage symptoms and limit complications [13].
These strategies may work better for some individuals than others. Always consult a qualified healthcare professional before starting any new supplement or exercise program.
Yes, research suggests there are overlapping genetic factors and comorbidities.
Shared features include sensory sensitivities, digestive problems, and coordination issues.
ADHD, anxiety, fibromyalgia, and mast cell activation syndrome (MCAS) are also reported in both conditions.
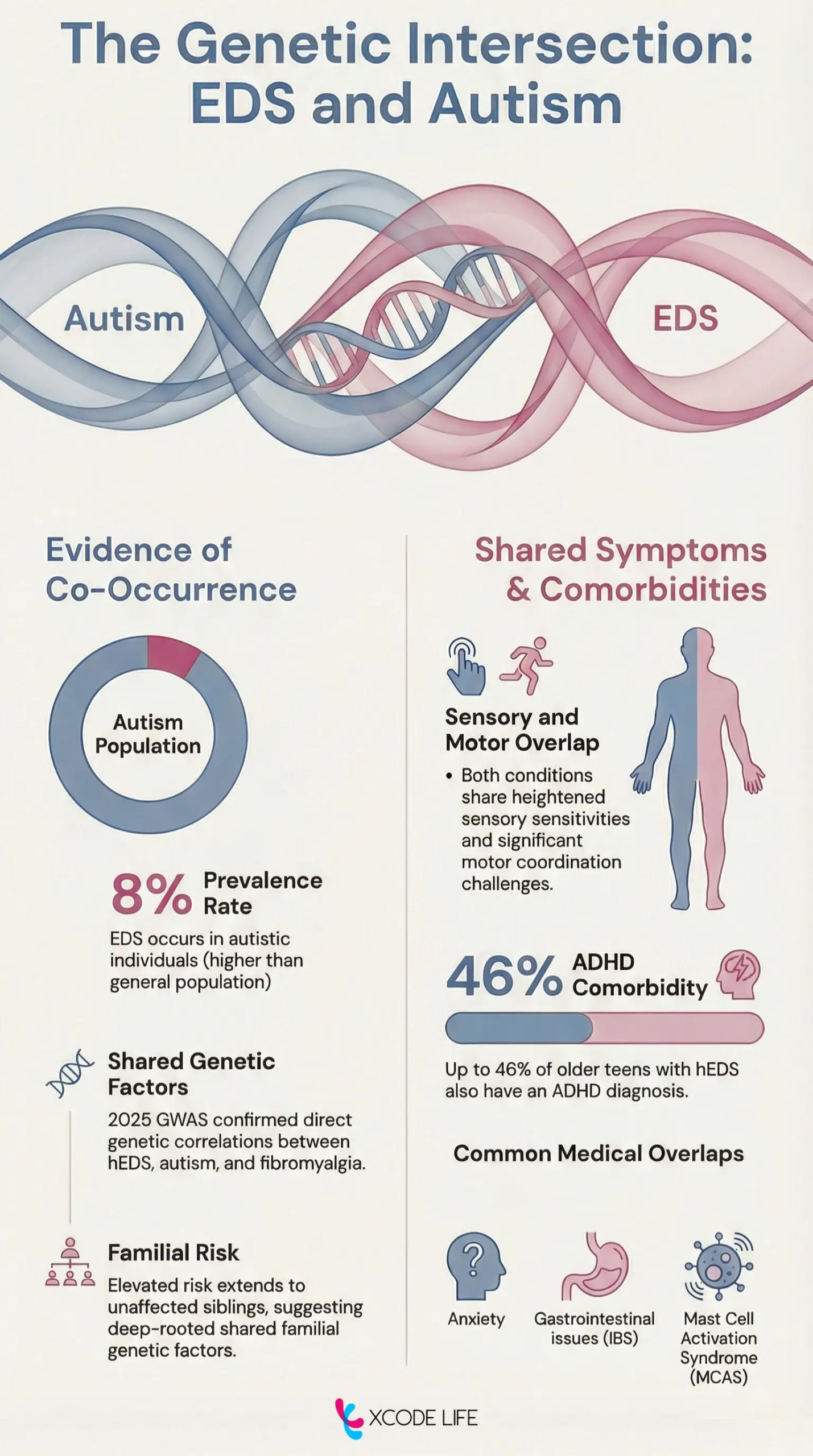
Symptomatically, both conditions share features such as:
**Proprioception is also called kinesthesia. It is the body's awareness of its position and movement in space, which is crucial for coordination and balance.
Mast Cell Activation Syndrome (MCAS): MCAS, more common in EDS, can cause flushing, GI issues, and chemical sensitivities. Some researchers are exploring whether similar immune responses occur in autism too.
Beyond hypermobile joints and stretchy skin, EDS can produce less-recognized symptoms, including chronic headaches (from craniocervical instability), bladder urgency, "brain fog" and cognitive difficulties, temperature dysregulation, and heightened sensitivity to medications or anesthesia. POTS-related dizziness and mast cell reactivity are also widely reported but often overlooked in diagnosis.
For most subtypes, including the most common hypermobile EDS, life expectancy is not shortened when symptoms are well-managed [20]. The exception is vascular EDS, where the median survival is approximately 51 years due to risks of arterial rupture and organ perforation, though outcomes are improving with celiprolol therapy and earlier diagnosis [21].
Yes. Flexibility may paradoxically decrease over time (as joints become more damaged), while chronic pain, fatigue, and joint instability often worsen. Connective tissue weakness can accumulate through repeated microtraumas, dislocations, and injuries over the years.
Key red flags that should prompt clinical evaluation include unusually flexible joints from childhood, a family history of similar symptoms, delayed wound healing, wide or "cigarette paper" scars, recurrent joint dislocations, and unexplained chronic pain or fatigue. In vascular EDS specifically, a family history of early-onset arterial rupture or organ perforation is a critical red flag requiring urgent genetic testing.
Yes, EDS can indirectly affect hair. Altered collagen and skin structure in EDS can lead to enlarged or disrupted hair follicles, which may affect hair quality and texture. Some patients report thinning brittle hair, which may also be linked to nutritional deficiencies common in EDS (such as iron, B12, or vitamin D) [22].
Certain features are more common in specific subtypes. In vascular EDS, affected individuals may have thin, translucent skin, a narrow or thin nose, a thin upper lip, small earlobes, and prominent eyes. Those with fair skin tone ay have prominently visible blood vessels [13]. In some rarer subtypes, structural features such as a high-arched palate, dental crowding, and small chin may be present.
Yes. Fragile connective tissue can make breast tissue more prone to pain, strain, or injury, particularly with changes in weight or posture. Ligamentous laxity around the chest can also contribute to musculoskeletal chest pain, which is commonly reported in hEDS.
EDS is frequently confused with Marfan syndrome, Loeys-Dietz syndrome, fibromyalgia, joint hypermobility syndrome/HSD, chronic fatigue syndrome, and even anxiety disorders. The average diagnostic delay for hEDS is several years to over a decade, in part because many clinicians are unfamiliar with the condition's systemic features [11].
Some individuals with EDS appear younger than their age due to soft, elastic skin, a reflection of altered collagen structure. However, the same collagen fragility that makes skin smooth also leads to easy bruising, scarring, and tissue damage over time.
Yes. EDS is a lifelong condition. Chronic pain is reported in approximately 90% of patients with hypermobile EDS [23], and management is centered on symptom control, joint protection, and quality of life rather than a cure.
EDS is a rare group of genetic conditions caused by collagen-related gene variants. Symptoms can range from joint instability and fragile skin to digestive problems and chronic fatigue. With 13 recognized types, hypermobile EDS is the most common. While EDS has no cure, early recognition, lifestyle support, and personalized medical care can greatly improve quality of life.
Estimated reading time: 6 minutes
Medications like Ozempic, Wegovy, Mounjaro, and Zepbound have completely transformed the landscape of weight loss and diabetes management. However, despite their soaring popularity, a significant number of people do not stay on them forever. In fact, research shows that nearly two-thirds of patients stop taking GLP-1 medications within a year[1]. Stopping Ozempic and Wegovy typically leads to a return of hunger and cravings[2]. Any improvements in blood sugar may also be reversed. All these put together can cause significant weight regain[3].
To understand what happens when you stop, it helps to know how these drugs work.
Medications like Ozempic (semaglutide) are GLP-1 receptor agonists.
They mimic a naturally occurring hormone in your body that regulates appetite and blood sugar.
The medication slows digestion, so your stomach empties more slowly, helping you feel fuller on smaller portions.
It also acts on the brain to suppress physical hunger and mental food cravings, often referred to as silencing "food noise".
what is the actual science behind GLP1 stopping food noise/obsession?
by u/Snoo_72731 in Semaglutide
Because obesity and diabetes are chronic conditions, GLP-1s are generally designed for long-term use. When the medication leaves your system, your body’s baseline biology returns.
The most common effect of stopping these medications is weight regain.
When you stop taking the drug, your digestion returns to baseline physiology.
The "food noise" and cravings can return, increasing the risk of overeating.
Clinical trials show that one year after stopping a maximum dose of semaglutide, individuals regain an average of two-thirds of the weight they lost[4].
Furthermore, research suggests that without the drug, weight regain usually happens in the form of fat, because fat is gained faster than skeletal muscle.
If you were prescribed Ozempic to manage type 2 diabetes, stopping the medication will likely cause your blood sugar levels to spike.
Ozempic works by helping the pancreas produce insulin when needed[5].
Without it, you may digest carbohydrates faster, and your body will not release insulin as efficiently, potentially leading to hyperglycemia.
Many people experience secondary health benefits while on GLP-1 medications, such as lower blood pressure and improved cholesterol levels[6].
Unfortunately, once the medication is stopped and weight begins to return, blood pressure and "bad" cholesterol levels often rise back to their pre-medication baselines[1].
There is a silver lining to stopping: the disappearance of unwanted side effects. Gastrointestinal issues like nausea, vomiting, diarrhea, and constipation are incredibly common on these medications[7].
Once the drug is out of your system, which can take a few days to a few weeks, these digestive side effects will naturally subside.
If these medications are so effective, why do so many people quit? The decision to stop is highly personal and often driven by:
| Expert picks: What To Read Next |
|---|
| Brello Health Review: Compounded GLP-1 Access Explained |
| Common And Rare Side Effects Of Semaglutide For Weight Loss |
If you are planning to stop your medication, you don't have to accept weight regain as an absolute certainty. With the right strategies, you can minimize the rebound effect:
Dr. John Marton, medical director of Bariatric Surgery at Yale New Haven Health says “Patients may have to stop taking GLP-1 medications because of side effects, affordability or lack of insurance coverage. However, it’s not a good idea to stop suddenly.”
Keeping weight off after ozempic is difficult, but not impossible. By tapering off gradually, following a healthy diet and workout routine, and managing stress and sleep, one may be able keep the weight off.
Stopping Wegovy (semaglutide) typically causes a return of appetite, increased "food noise" (constant thoughts about food), and gradual weight regain, as the medication's appetite-suppressing effects wear off over 5 to 7 weeks[9].
It is not recommended to stop semaglutide cold turkey. However, your doctor may stop your medication immediately in case of any medical emergency or sever side effects.
Ozempic hands refers to an informal, non-medical term used to describe the loss of fat under the skin on your hand. This leads to a more “skeletal” and “bony” appearence with prominent veins.
To minimize weight regain after discontinuing Ozempic, the dose should be gradually reduced with guidance from a healthcare professional instead of stopping suddenly. Preserving weight loss depends on continuing habits such as a protein-forward, high-fiber diet, regular strength training, and staying alert to the reappearance of increased appetite or “food noise.” Sustainable, long-term lifestyle adjustments are key to counteracting the return of appetite-regulating hormones.
Some rare but potentially permanent and serious side effects include pancreatitis, gall bladder issues like gall stones, stomach paralysis, and some vision conditions like retinopathy, macular degeneration, and NAION[10].
Stopping medications like Ozempic or Wegovy can trigger significant physiological shifts, including a return of appetite and changes in blood sugar. If you are considering discontinuing your medication, always consult with your healthcare provider first. They can help you create a personalized exit strategy, which may include tapering your dose, adjusting your diet, or exploring alternative treatments to help you sustain your hard-earned health results.